This document provides information on deep vein thrombosis (DVT), including:
- DVT occurs when a blood clot forms in a deep vein, most often in the leg. Part of the clot can break off and cause a pulmonary embolism.
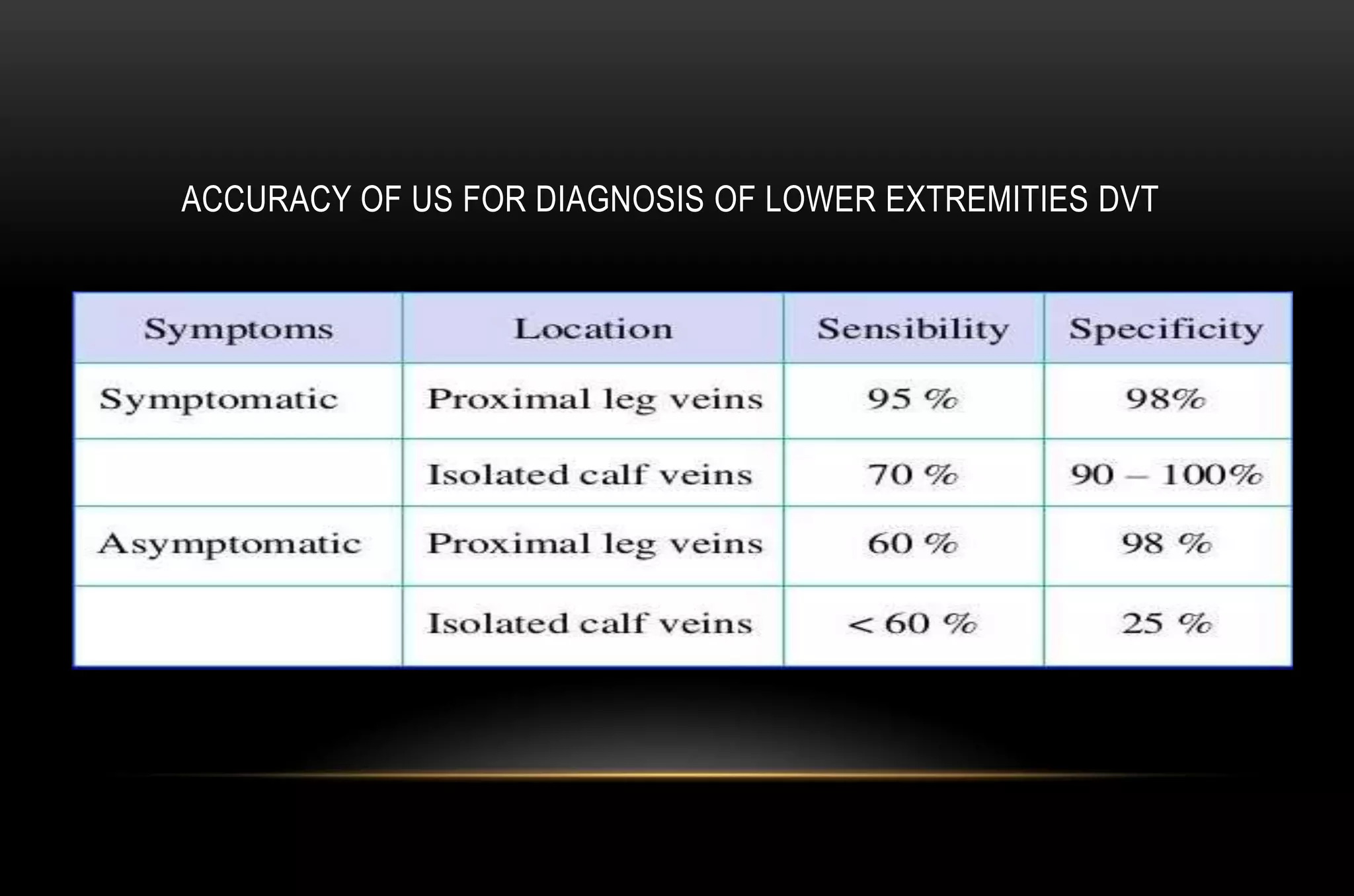
- Risk factors include pregnancy and immobilization. Ultrasound is the main imaging method used to diagnose DVT.
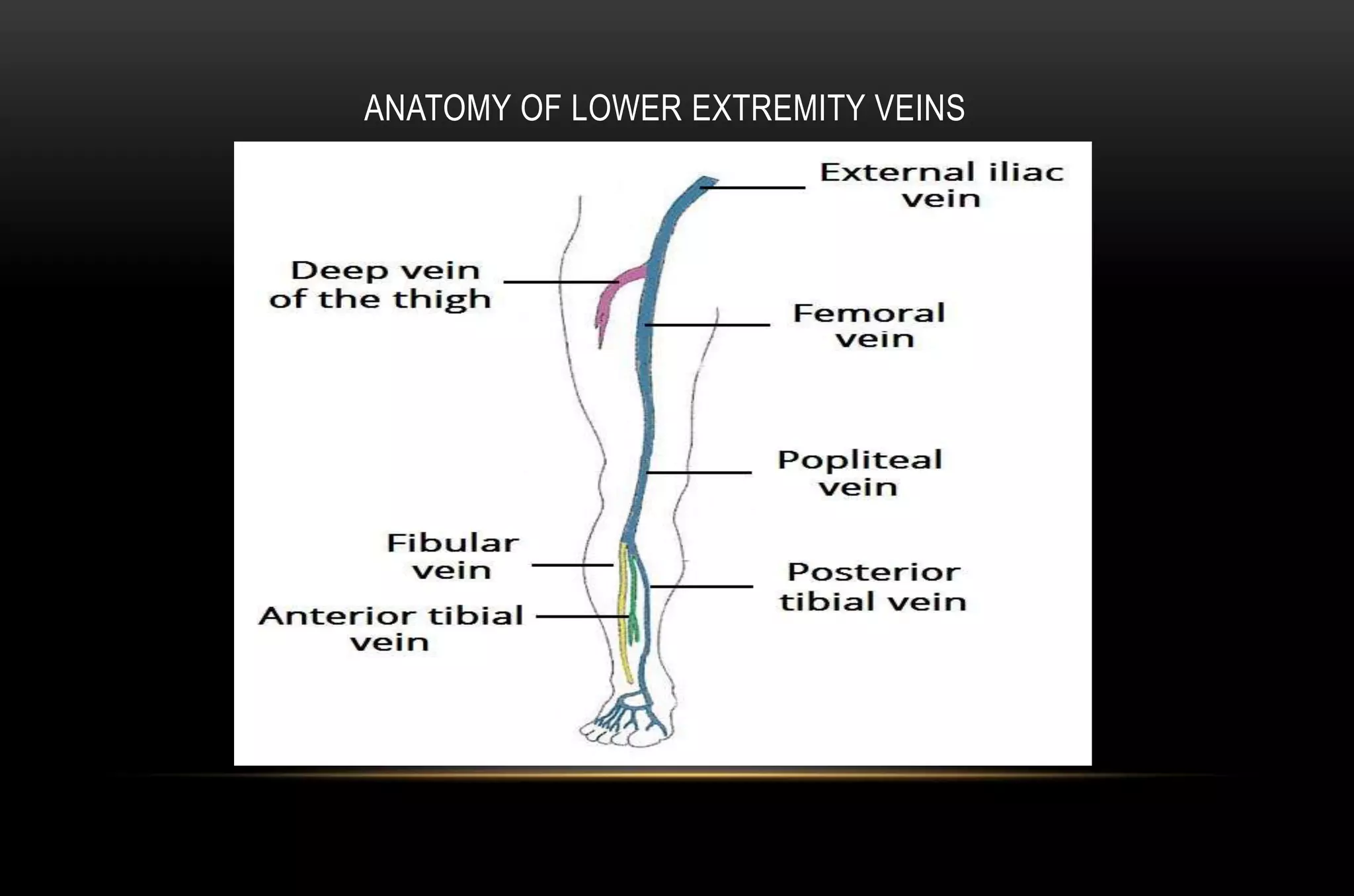
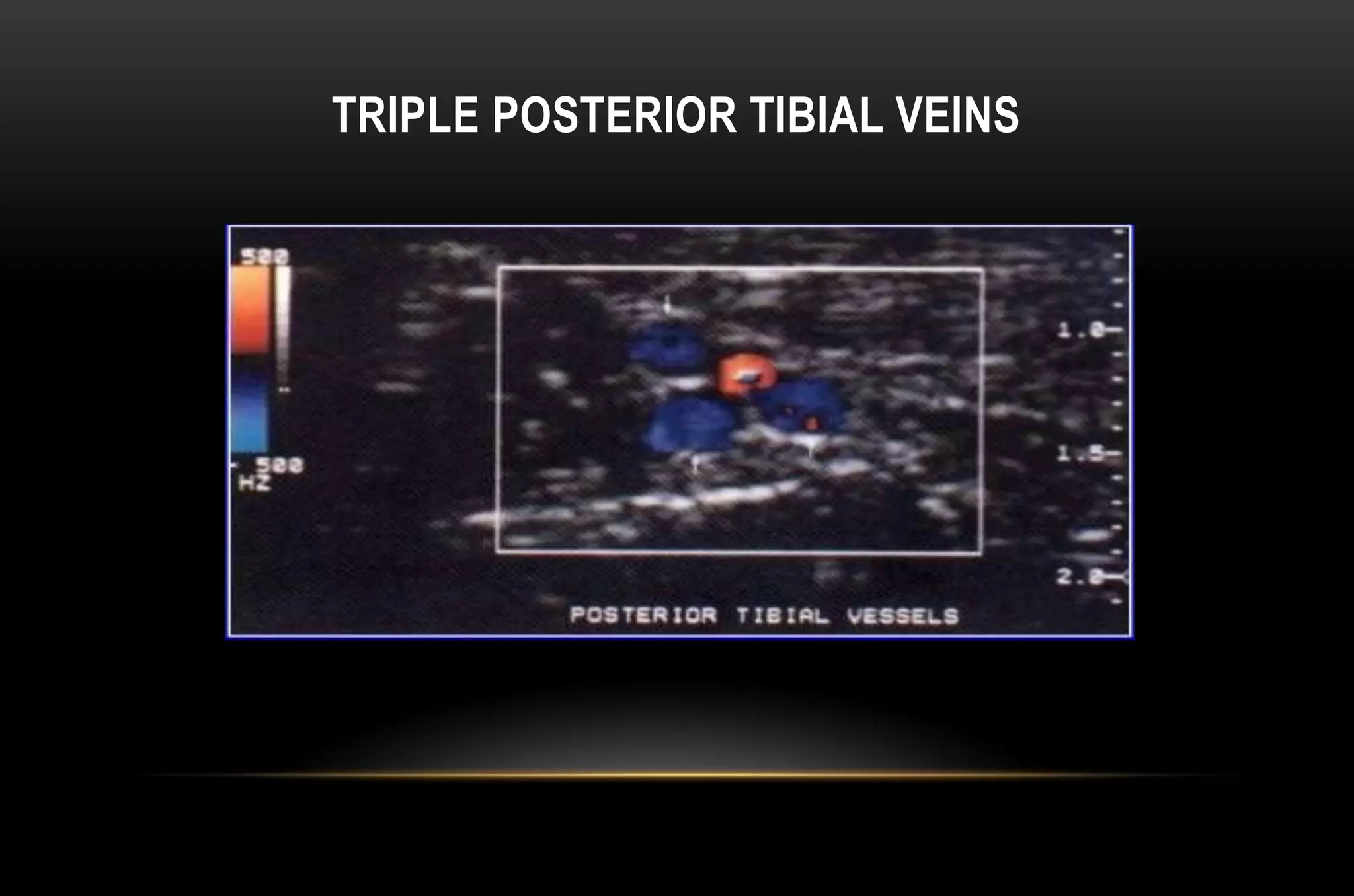
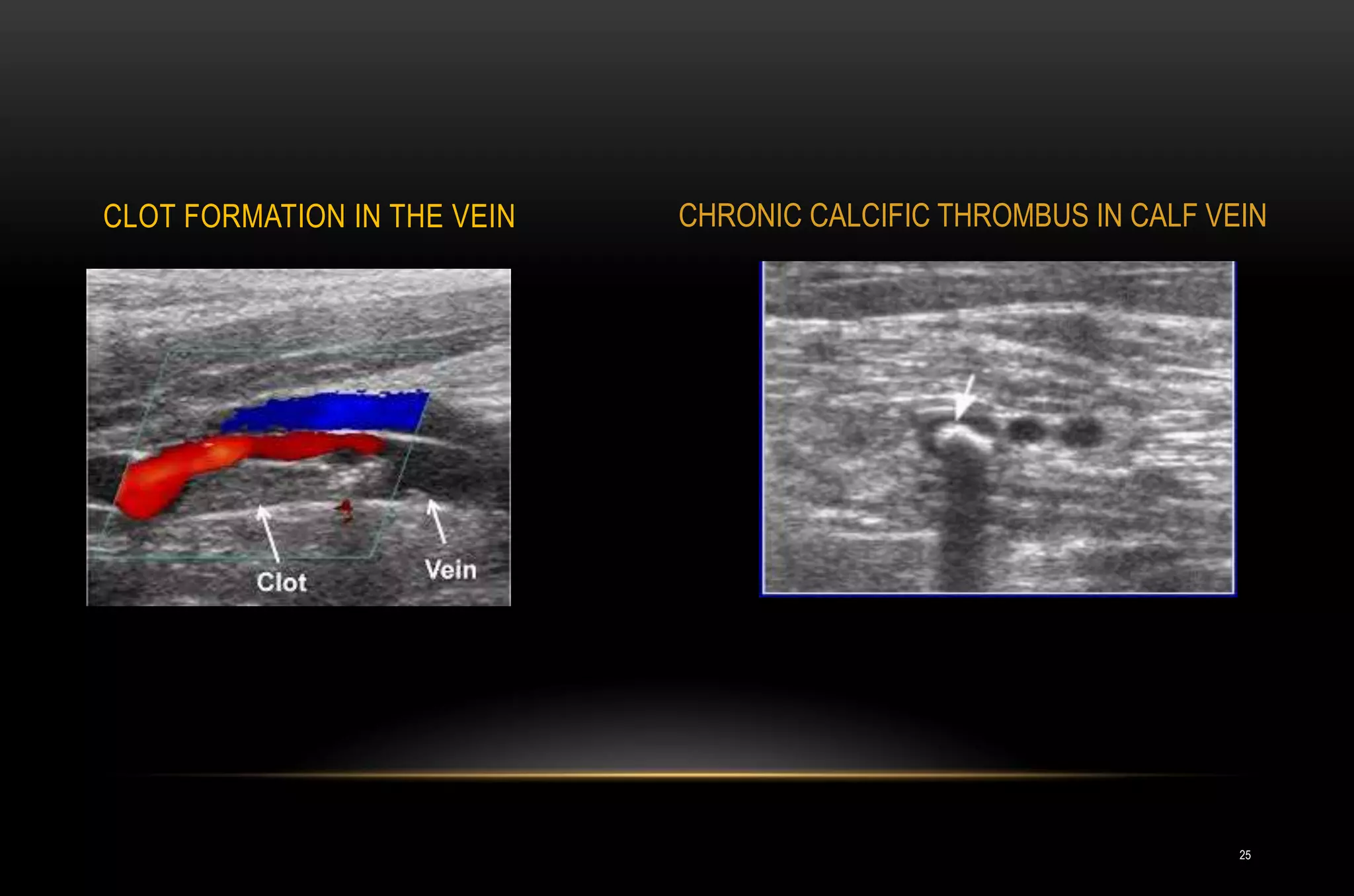
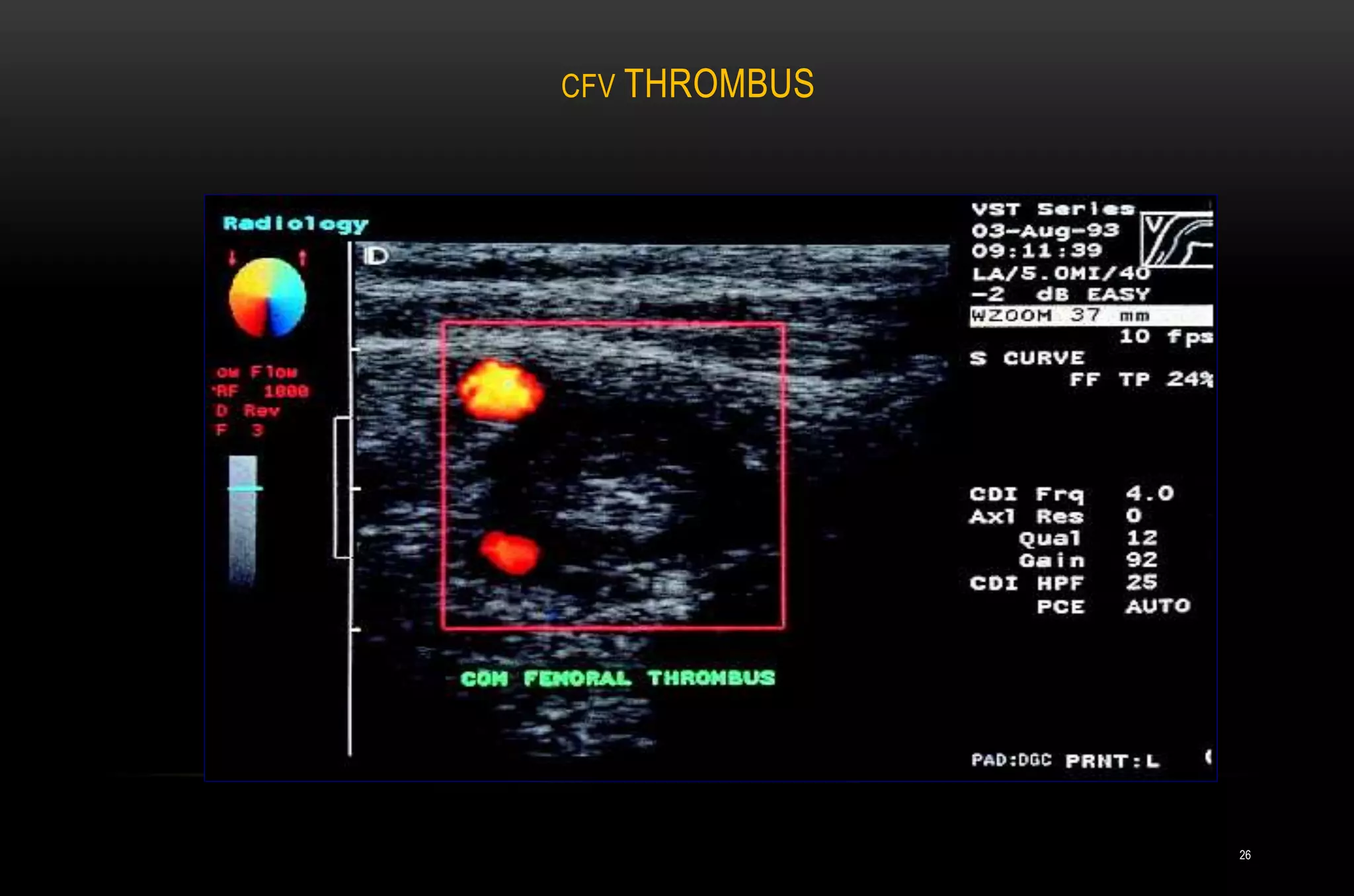
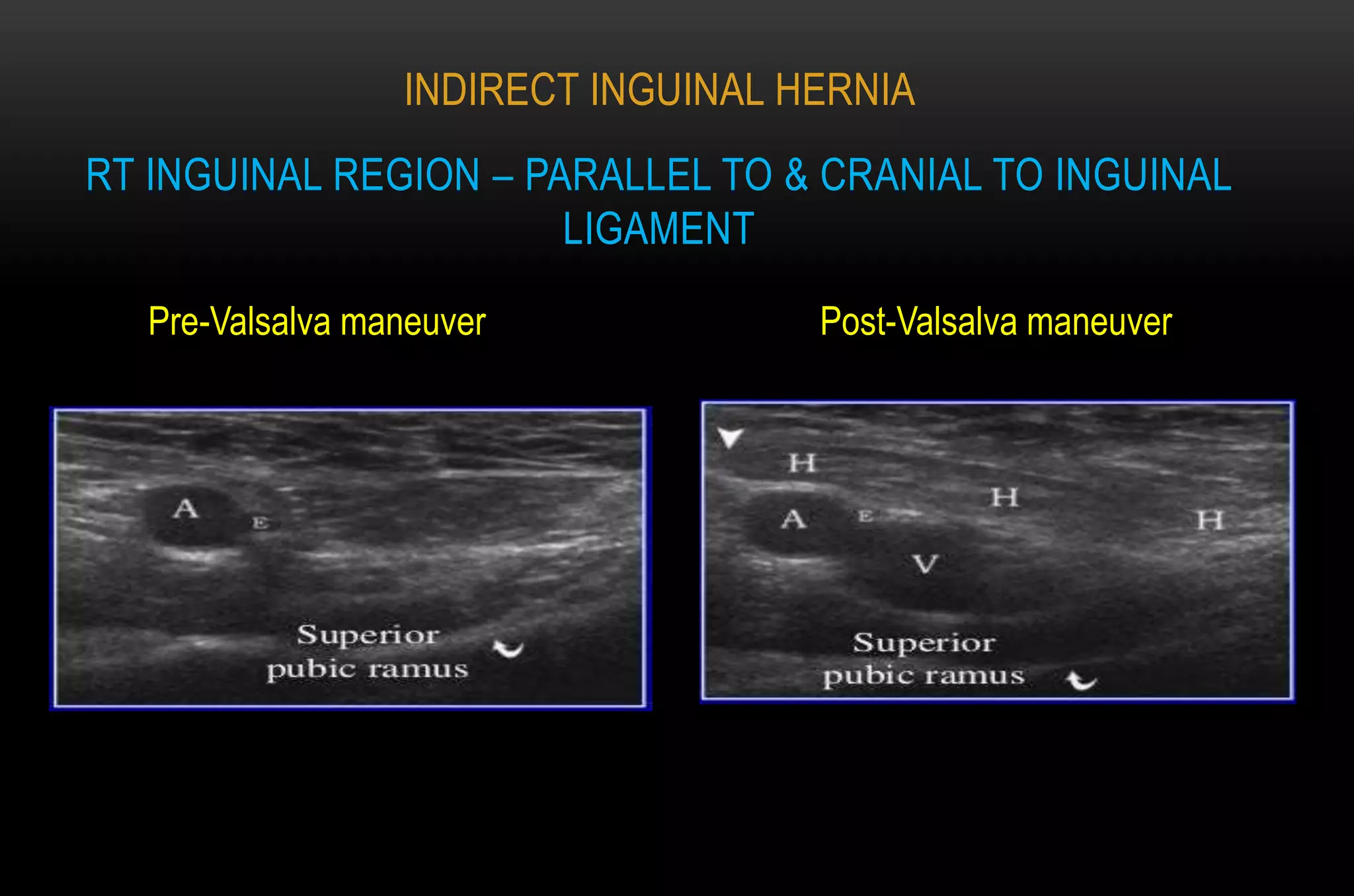
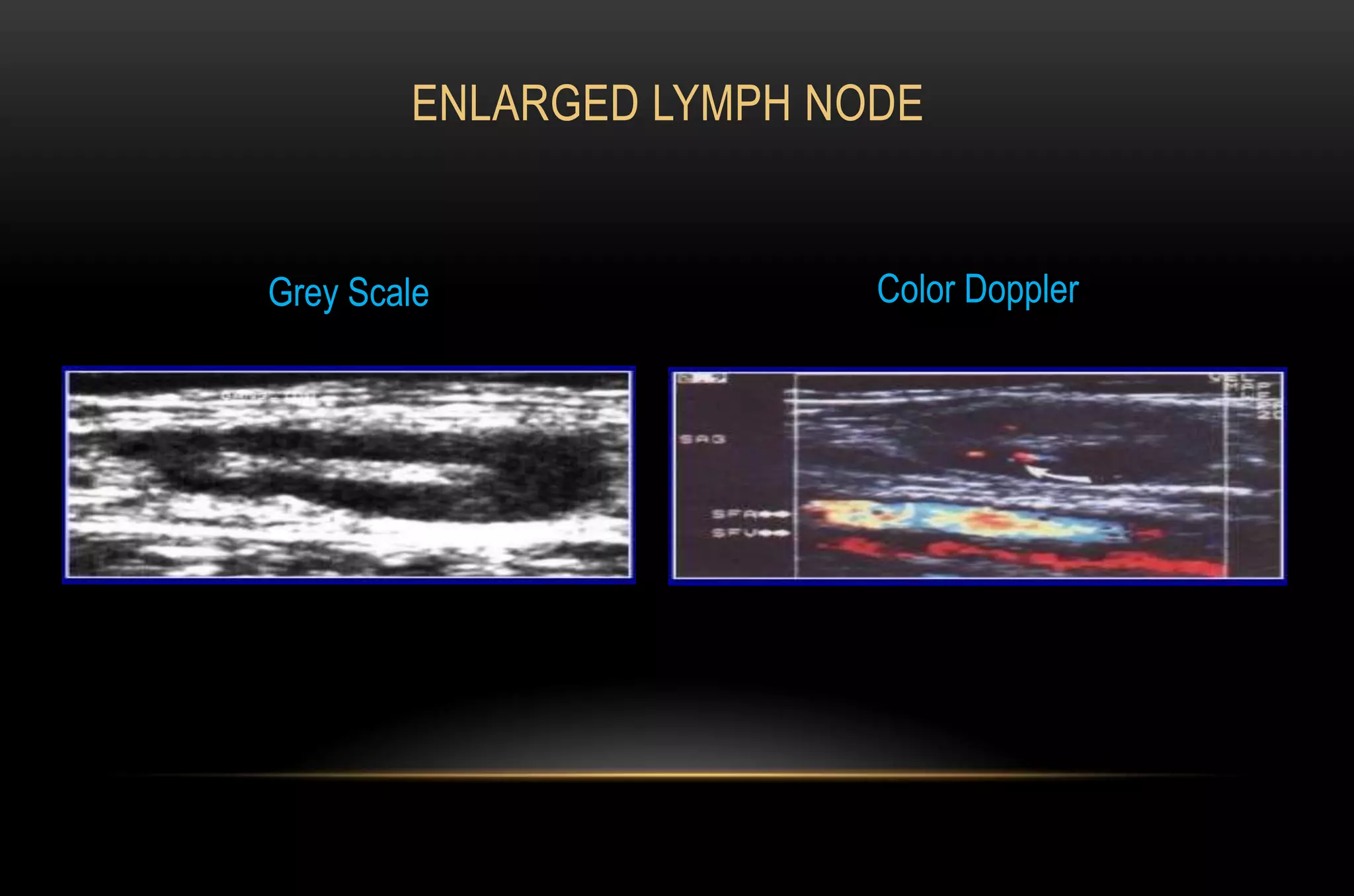
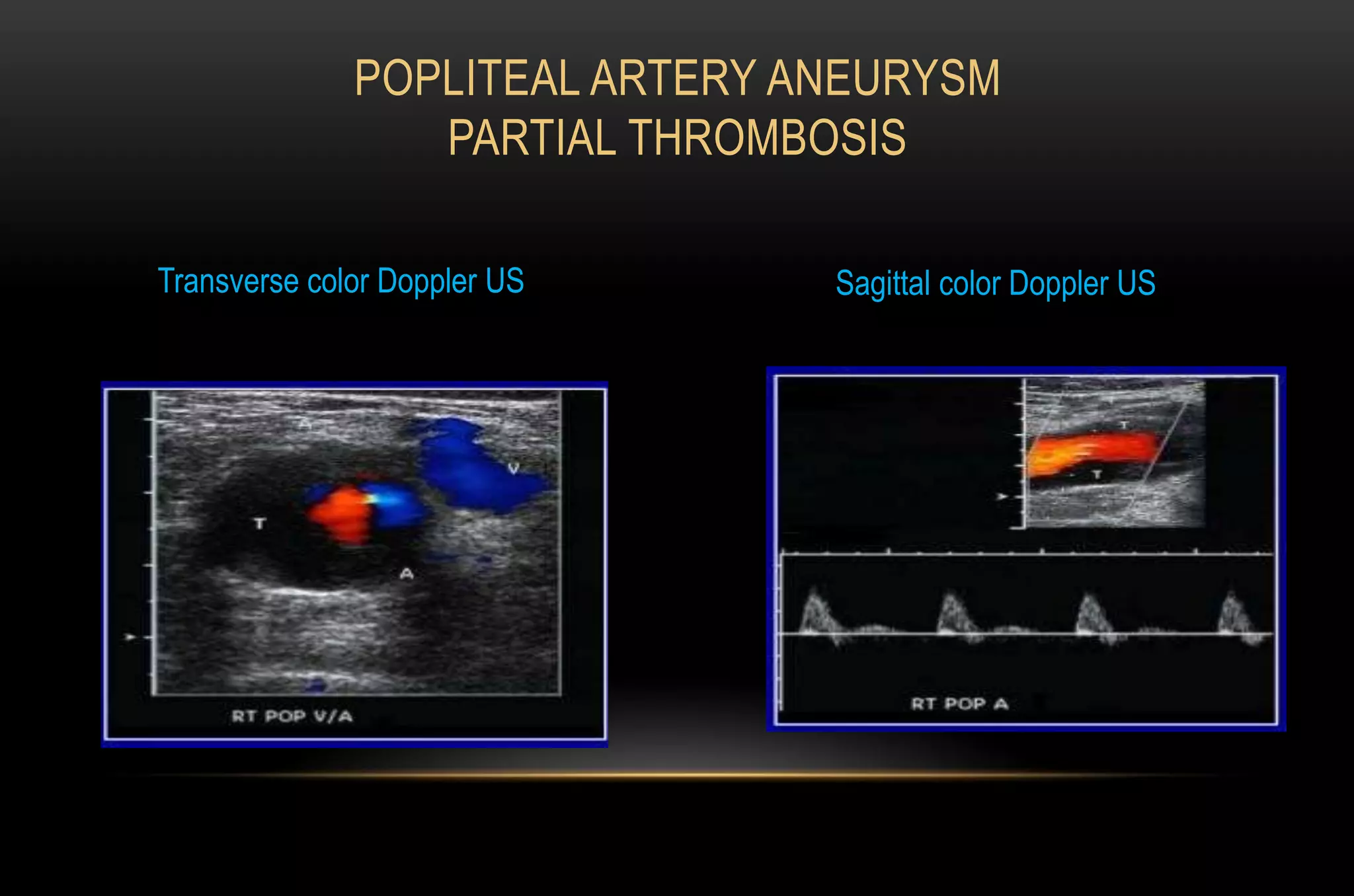
- Ultrasound findings of DVT include non-compressible veins, lack of flow, and visualization of thrombus within the vein. Differential diagnoses when DVT is ruled out include muscle injuries, hernias, cysts, and arterial diseases. Proper patient positioning and knowledge of anatomy are important for accurate ultrasound evaluation.