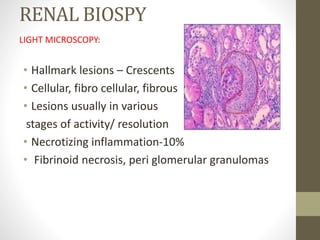
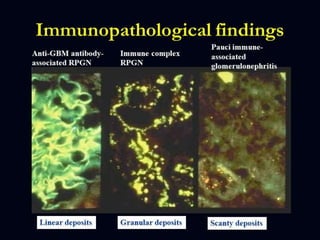
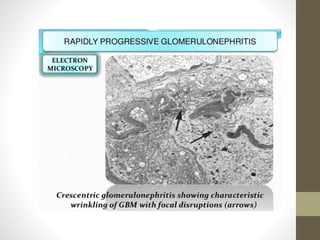
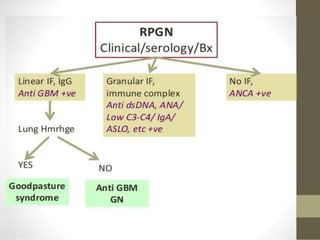
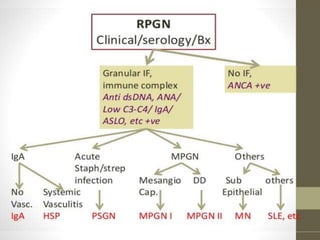
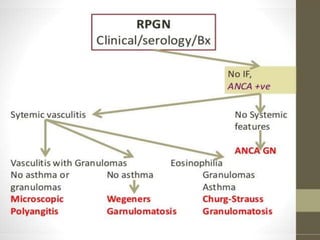
Rapidly progressive glomerulonephritis (RPGN) is characterized by a rapid loss of renal function over a short period of time. It is classified as primary or secondary RPGN based on its underlying causes. The pathogenesis involves crescent formation in glomeruli due to proliferation of cells and inflammation. Clinically, it presents with hematuria, proteinuria, hypertension, and declining kidney function. Diagnosis involves lab tests showing abnormalities in urine, blood counts, complement levels, and antibodies. Renal biopsy revealing crescentic lesions in glomeruli is diagnostic. Treatment depends on the specific type but often includes steroids, plasmapheresis and cyclophosphamide to slow kidney damage. Prognosis depends