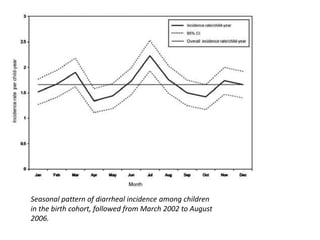
This document summarizes a study on rotavirus and other causes of diarrhea in children in a southern Indian community. The study followed 452 newborn infants for 3 years, monitoring diarrhea incidence through twice weekly home visits. A total of 1856 diarrhea episodes were recorded. Rotavirus was found to be the most common cause, associated with 18% of episodes. Other common causes included Giardia (8%) and Aeromonas (4%). Diarrhea incidence was highest in infancy, at 1.6 episodes per child on average over 3 years. Poor hygiene was associated with more severe diarrhea. The study provides valuable community-level data on the etiology and burden of childhood diarrhea in southern India.