Download as PDF, PPTX
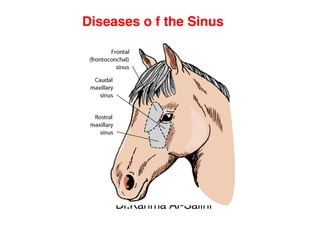
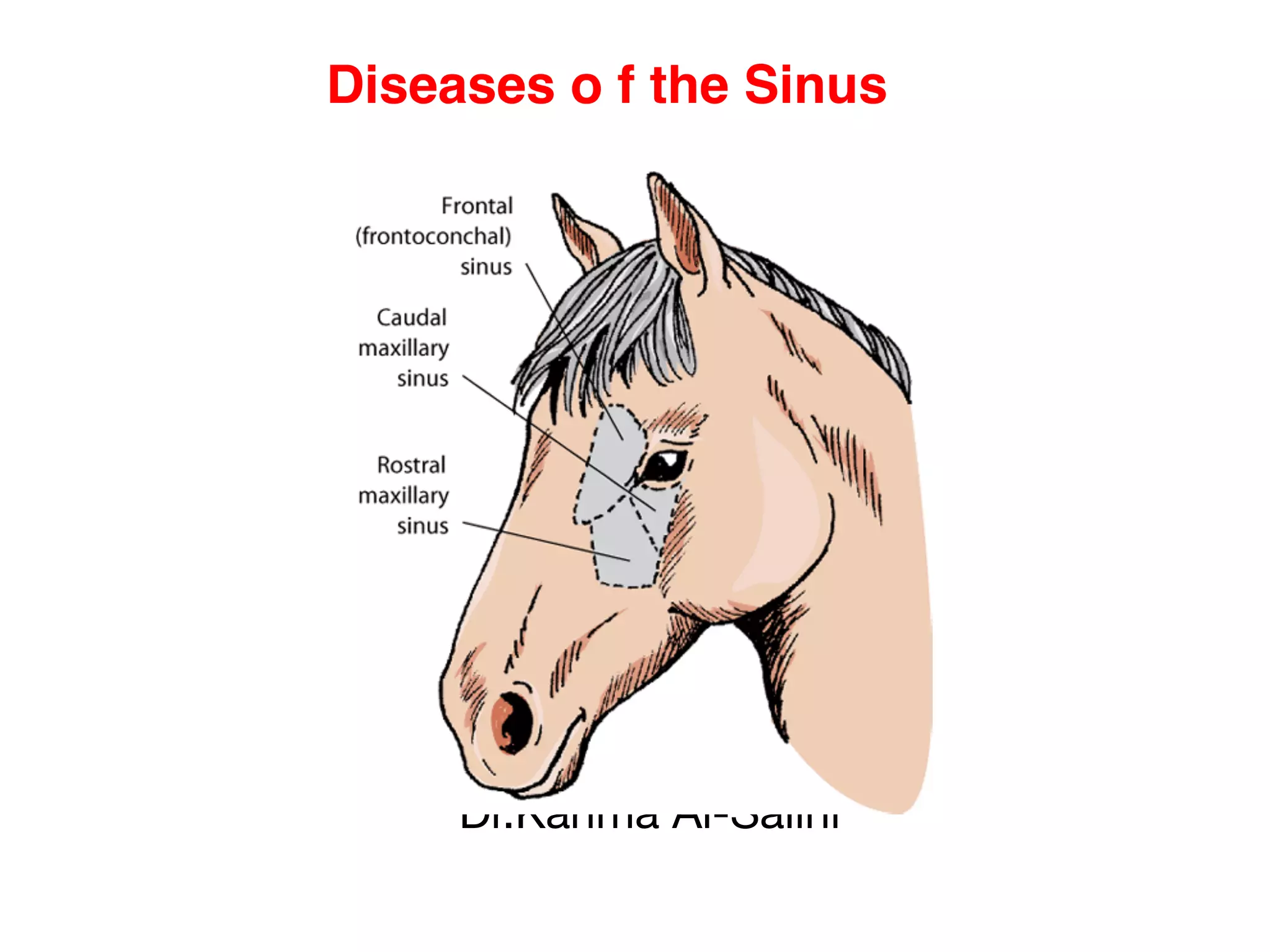
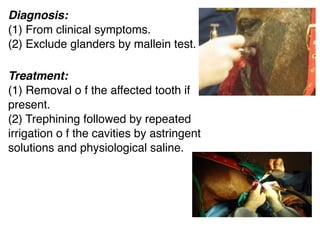

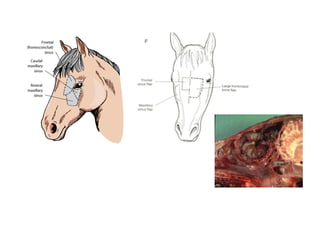

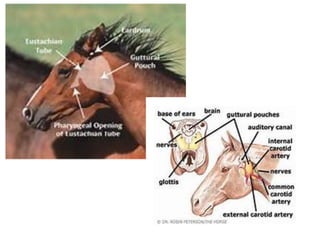
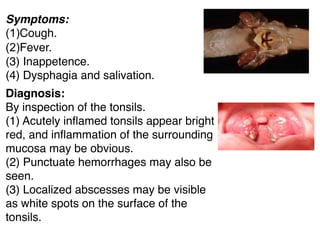
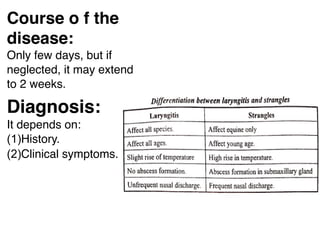
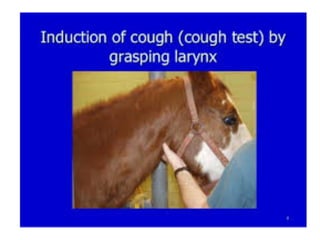

This document discusses several diseases of the sinus and respiratory tract in animals. It describes catarrh of the maxillary sinus and frontal sinus, which cause nasal discharge and tenderness over the affected area. Catarrh of the guttural pouch can lead to complications like stenosis of the larynx. Tonsillitis in pets is usually caused by Streptococcus and causes cough, fever, and dysphagia. Laryngitis and trachitis produce a dry, harsh cough and respiratory distress due to inflammation of the airways. Treatment involves removing the underlying cause, antibiotics, anti-inflammatories, and in some cases surgery.





![Respimicro [recovered]](https://cdn.slidesharecdn.com/ss_thumbnails/respimicrorecovered-110909043628-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)















































































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)

