Downloaded 85 times

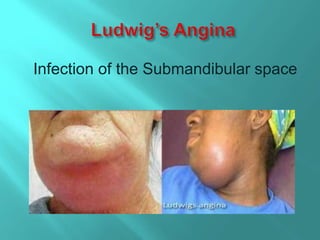
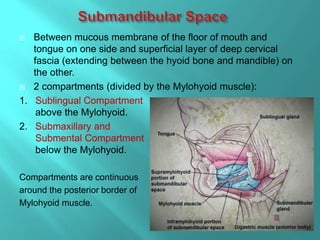
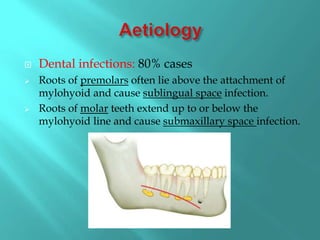



This document discusses infections of the submandibular space, which is divided into two compartments by the mylohyoid muscle. Dental infections are the most common cause, with roots above or below the mylohyoid muscle leading to sublingual or submaxillary infections, respectively. Symptoms include odynophagia, trismus, and swelling of the submental and submandibular regions. Treatment involves systemic antibiotics, incision and drainage of any abscesses either intraorally or externally, and tracheostomy if the airway is endangered. Complications can arise from spread of infection or airway obstruction.





































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







