Downloaded 11 times

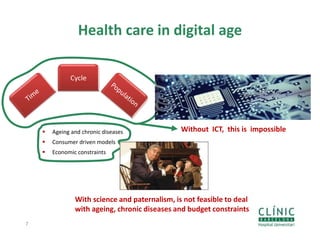

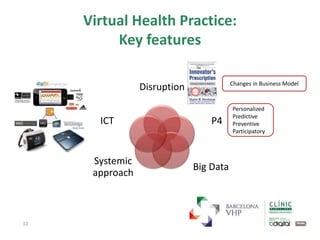
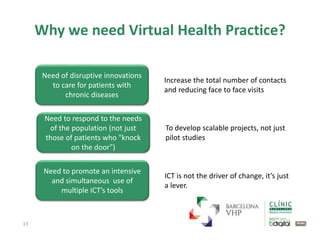





1) The document discusses the need for increased patient participation and a virtual health practice model to deal with challenges of an aging population, consumer driven models, and economic constraints. 2) It proposes a virtual health practice strategy that promotes consistent use of technology across the care cycle to increase patient contact, reduce face-to-face visits, and maximize health outcomes in a sustainable way. 3) The key features of virtual health practice are that it is personalized, predictive, preventive, participatory, and relies on disruptive innovations using big data and multiple ICT tools in a systemic approach.












































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















