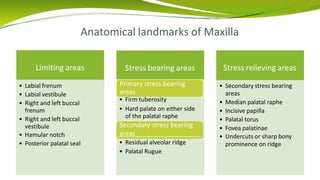
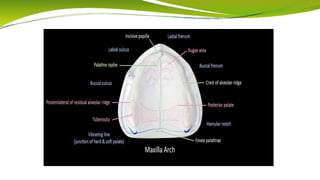
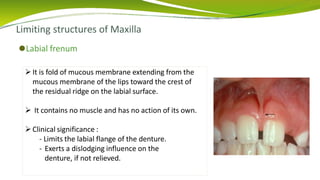
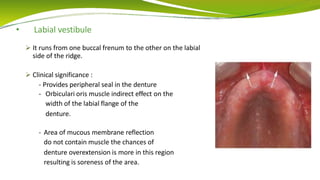
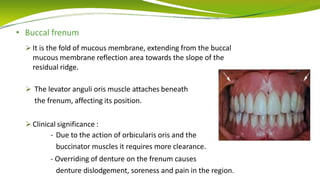
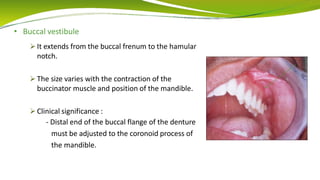
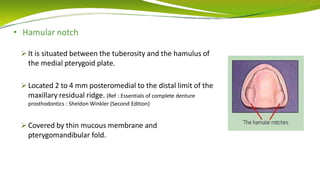
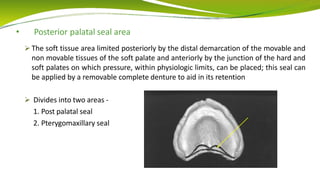
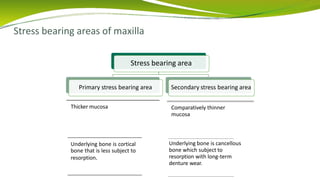
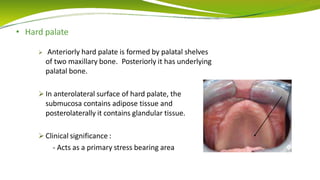
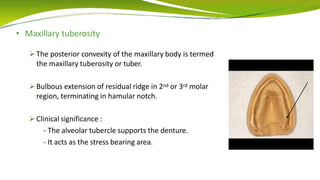
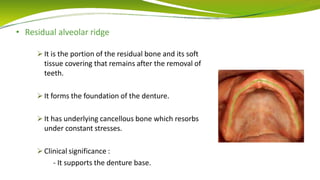
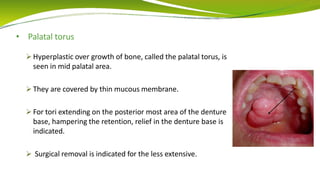
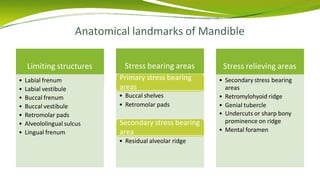
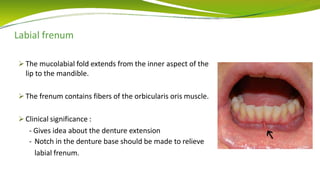
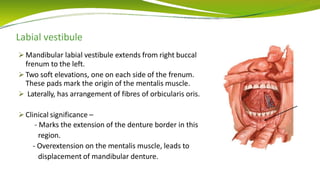
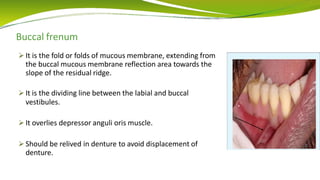
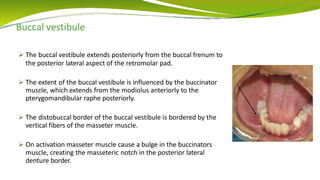
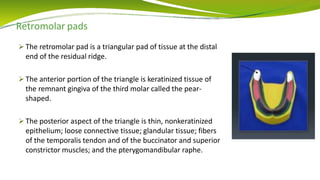
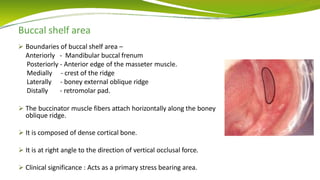
This document discusses anatomical landmarks that are important for complete dentures. It defines landmarks as recognizable anatomic structures used as reference points. The maxilla and mandible each have limiting structures that determine the denture border, supporting structures that tolerate biting forces as foundations for the denture, and stress relieving structures that should be relieved in the denture due to being fragile or prone to resorption. Specific maxillary landmarks include the labial and buccal frenums, hard palate, and tuberosity. Mandibular landmarks include the labial frenum, buccal shelves, and residual ridge. Understanding these landmarks is crucial for achieving proper retention, stability, and support of complete dentures.

































![Anatomical landmarks of maxilla and mandible [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anatomicallandmarksofmaxillaandmandibleautosaved-200820132830-thumbnail.jpg?width=640&height=640&fit=bounds)


























![001 Enamel hypoplasiaffd [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/001enamelhypoplasiaautosaved-241025222519-c23f3c11-thumbnail.jpg?width=640&height=640&fit=bounds)






















