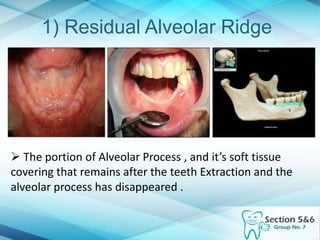
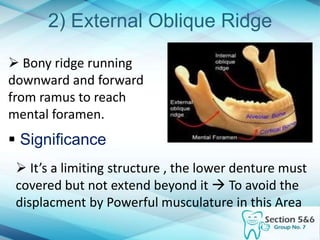
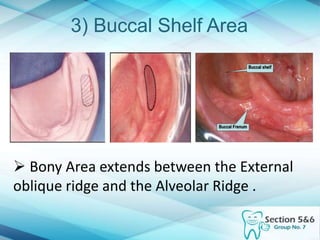
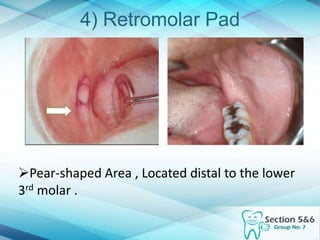
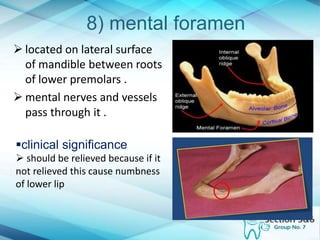
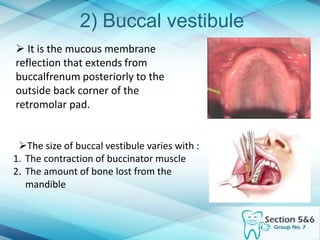
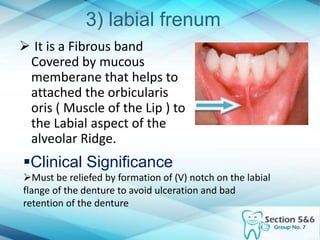
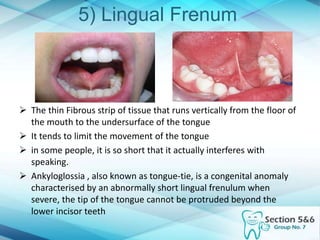
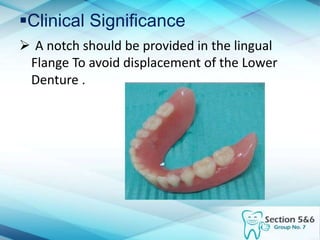
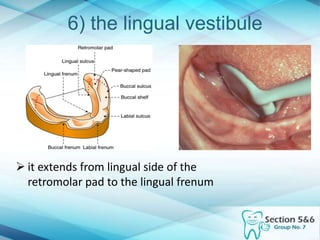
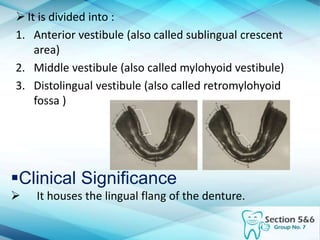
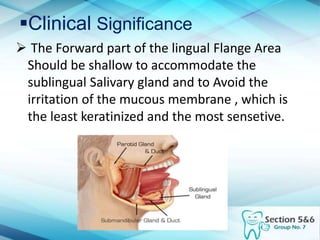
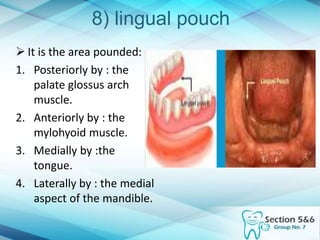
The document discusses intraoral landmarks that are important for denture construction and placement. It describes supporting structures like the residual alveolar ridge and limiting structures like the buccal frenum. Each structure is explained, including its anatomical features and clinical significance for ensuring proper denture fit, retention, and avoidance of irritation or injury. In summary, the document provides details on key intraoral structures that dentists must consider when fabricating removable dentures.