
Recommended
More Related Content
What's hot
What's hot (20)
Similar to 16 Spinal Cord And Spinal Nerves
Similar to 16 Spinal Cord And Spinal Nerves (20)
More from guest334add
More from guest334add (16)
Recently uploaded
Recently uploaded (20)
16 Spinal Cord And Spinal Nerves
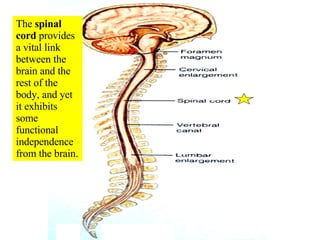
- 1. The spinal cord provides a vital link between the brain and the rest of the body, and yet it exhibits some functional independence from the brain.
- 2. The adult spinal cord travels from the foramen magnum and terminates within the vertebral foramen of the first lumbar vertebra (L1) in adults.
- 3. The spinal cord can be subdivided into five regions: cervical region, thoracic region, lumbar region, sacral region, and coccygeal region (which has only one pair of nerves). Don’t be confused and think that the sacral “region” of the spinal cord is surrounded by sacral vertebrae. It is NOT!
- 4. The diameter of the spinal cord is the largest in the cervical region and there is a larger proportion of white matter compared to gray matter.
- 5. The diameter of the sacral region of the spinal cord (which is surrounded by the T12/L1 vertebrae) is the smallest and the proportion of gray matter is largest in the spinal cord.
- 6. The cervical enlargement contains the neurons that innervate the upper limbs The lumbar enlargement contains the neurons that innervate the lower limbs.
- 7. The tapering end of the spinal cord is called the conus medullaris . The conus medullaris is surrounded by L1 in and adult and L2 in a child .
- 8. The adult spinal cord terminates at the level of the first lumbar vertebra (L1) In a developing child , the spinal cord can extend to the level of the second lumbar vertebra (L2)
- 9. The cauda equina (horse’s tail) is composed of nerves that arise from the conus medullaris and extend inferiorly.
- 10. The filum terminale , which is composed of pia mater, extends from the conus medullaris to the coccyx. Note the subarachnoid space also continues for some distance.
- 11. There are 31 pairs of spinal nerves that serve defined segments of the human body.
- 12. There are 8 pairs of cervical spinal nerves. This is possible because the first pair (C1 spinal nerves) exits the spinal column between the occipital bone and the atlas (C1). The remaining 7 pairs (C2-C8 spinal nerves) exit below each of the 7 cervical vertebrae via the intervertebral foramina. All the spinal nerves are mixed nerves.
- 13. The spinal cord is surrounded by the dura, arachnoid, and pia maters (the meninges)
- 14. WHAT IS THE NAME OF THE NERVE THAT EXITS VIA THE INTERVERTEBRAL FORAMEN BETWEEN THE ATLAS AND THE AXIS? A VAGUS NERVE B FIRST CERVICAL SPINAL NERVE C ACCESSORY NERVE D LONG THORACIC NERVE E SPINAL NERVE C2
- 15. The epidural space is between the vertebra and the dura mater
- 18. Effect of epidural anesthesia
- 19. A person who needs an epidural!
- 20. The dura mater extends along the entire length of the vertebral canal and surrounds the spinal cord. It also extends along the initial portion of the radiating spinal nerves
- 21. The subarachnoid space is a real space filled with CSF
- 22. In this midsagittal picture #3 is the dura mater, #5 is the spinal cord, # 4 is the epidural space, and #6 is the subarachnoid space where CSF is located (#1 is an intervertebral disc and #2 is the body of a vertebrae).
- 23. Needle for spinal tap
- 24. Spinal taps are done between the third and fourth lumbar vertebrae because there is no spinal cord at that location
- 25. The tip of the needle is inserted into the subarachnoid space outside the cauda equina and spinal fluid is removed for testing.
- 26. The entering pressure can be determined when the needle is inserted into the subarachnoid space during a spinal tap.
- 27. Spinal fluid is normally crystal clear like water. Cloudy spinal fluid, like the specimen shown, is a sign of white blood cells (pus). The most common cause for white blood cells in the spinal fluid is viral or bacterial meningitis.
- 28. The pia mater directly adheres to the spinal cord
- 29. WHICH OF THE FOLLOWING IS TYPICALLY PENETRATED DURING A ROUTINE SPINAL TAP? A PIA MATER B NUCLEUS PULPOSUS C ANULUS FIBROSUS D SPINAL CORD E NONE OF THE ABOVE
- 30. The cross-sectional view shows that the gray matter is central and the white matter is peripheral
- 31. The peripheral white matter contains ascending and descending tracts of nerves traveling to and from the brain. The central gray matter serves as a center for spinal reflexes.
- 32. The central canal runs the entire length of the spinal cord, is contiguous with the brain and contains cerebrospinal fluid (CSF)
- 33. The spinal cord develops as 31 segments , each of which gives rise to a pair of spinal nerves that emerge from the cord through the intervertebral foraminae
- 34. Nerves can be sensory, motor, or mixed (sensory and motor)
- 35. Mixed nerves carry both types of information and some axons are transmitting impulses in one direction, while other axons are transmitting impulses in the opposite direction. All spinal nerves are mixed nerves.
- 36. There are 8 pairs of cervical spinal nerves. This is possible because the first pair (C1 spinal nerves) exits the spinal column between the occipital bone and the atlas (C1). The remaining 7 pairs (C2-C8 spinal nerves) exit below each of the 7 cervical vertebrae via the intervertebral foramina. All the spinal nerves are mixed nerves.
- 37. Most of the spinal nerves are associated with specific dermatomes (an area of skin innervated by all the cutaneous neurons of a certain spinal or cranial nerve).
- 38. Dermatome map. Note the trigeminal nerve has dermatomes on the face. trigeminal
- 39. Dermatomes of the trigeminal nerve (cranial nerve V) are seen on the face
- 40. Note that the trigeminal nerve has dermatomes on the face (see white area) and that the first pair of cervical spinal nerves (C1 spinal nerves) are not represented on the surface at all.
- 42. Chickenpox (varicella) virus is acquired by the respiratory route and causes a head-to-toe rash in children . The chickenpox virus can invade the ganglia along the spinal cord and remain latent until adulthood. It can then be activated by suppression of the immune system. It will then travel through sensory axons of a single dermatome and erupt onto the skin in a single dermatome on one side of the body (unilateral eruption)
- 43. Shingles is a reactivation of latent chickenpox from childhood that travels to the surface via a single nerve on one side of the body.
- 44. Shingles involving the first (ophthalmic) division of the trigeminal nerve (cranial nerve V) on face.
- 45. Explanation of referred pain . Numerous cutaneous and visceral sensory neurons share the same ascending tracts.
- 46. Body diagram of where referred pain may be felt.
- 47. WHICH OF THE FOLLOWING IS CORRECT ABOUT SHINGLES? A ADULTS WITH THIS CONDITION CAN CAUSE A HEAD-TO-TOE RASH IN CHILDREN B IT TYPICALLY OCCURS BILATERALLY C IT IS TRIGGERED BY ETHYL ALCOHOL AND PROLONGED NERVE COMPRESSION D IT IS MOST COMMON IN PERSONS UNDER 50 E ALL OF THE ABOVE
- 48. The majority of the spinal nerves combine and then split again as networks of nerves referred to as plexuses. The exceptions are T2-T12 and S5-Co1, which do NOT form plexuses
- 49. The cervical plexus is formed primarily by spinal nerves C1-C4 (C5 is not considered part of this plexus, even though it contributes some axons)
- 50. The cervical plexus, and particularly spinal nerves C3, C4, and part of C5, give rise to the phrenic nerve which innervates the diaphragm . Injury above C3 would lead to death by suffocation.
- 51. The brachial plexus is formed primarily by spinal nerves C5-C8, and T1. This plexus gives rise to five nerves that serve the arm or hand.
- 52. There are five nerves that arise from the brachial plexus
- 53. The axillary nerve innervates the teres minor muscle and the deltoid muscle. It receives sensory information from the superolateral part of the arm and skin.
- 54. The median nerve innervates muscles in the antebrachium and manus. It receives sensory information from the palmar side of fingers #1, #2, #3, and the lateral one-half of finger #4 and from the dorsal tips of these same fingers.
- 57. Note adduction of thumb
- 59. When draping my arm around my daughter’s neck for prolonged periods I would develop anesthesia of fingers #1-#4 only from pressure on my median nerve.
- 60. The musculocutaneous nerve innervates the biceps brachii muscle and several other muscles. It receives sensory input from the lateral surface of the forearm.
- 61. The radial nerve innervates the triceps brachii and numerous muscles of the antebrachium. It receives sensory input from the posterior arm and forearm surface and the dorsolateral side of the hand.
- 62. The radial nerve receives sensory input from the posterior arm and forearm surface and the dorsolateral surface of the hand .
- 63. The ulnar nerve , which passes near the medial epicondyle of the humerus, is the “funny bone”. It innervates muscles in the antebrachium and manus. It receives sensory input from the skin of the dorsal and palmar aspects of fingers #5, and the medial half of finger #4.
- 64. The ulnar nerve receives sensations from the skin of the dorsal and palmar surfaces of fingers #5 and medial half of fingers #4.
- 65. Atrophy of the arm muscles caused by a brachial plexus injury in adulthood. Read about brachial plexus injuries in the clinical view in your text.
- 66. A PATIENT HAS SUFFERED A FRACTURE OF THE SURGICAL NECK OF THE FEMUR THAT IS SUCCESSFULLY REPAIRED WITH A MEDULLARY ROD THAT BRIDGES THE FRACTURE LINE. HOWEVER, AS THE WEEKS PASS, THE PATIENT IS UNABLE TO ABDUCT THE ARM AND SUFFERS FROM ANESTHESIA ALONG THE SUPEROLATERAL SKIN OF THE ARM . WHAT HAS BEEN DAMAGED? A MEDIAN NERVE B MUSCULOCUTANEOUS NERVE C AXILLARY NERVE D ULNAR NERVE E RADIAL NERVE
- 67. The lumbar plexus is formed by spinal nerves L1-L4. It gives rise to two major nerves: the femoral nerve and the obturator nerve
- 68. Note the two major nerves that arise from the lumbar plexus
- 69. The femoral nerve innervates the quadriceps femoris muscles on the anterior of the thigh to help extend the knee. It also innervates the sartorius muscle and several other muscles. It receives sensory input from the anterior and inferomedial thigh as well as the medial aspect of the leg.
- 70. The obturator nerve innervates the gracilis and several other muscles. It receives sensory information from the superomedial skin of the thigh
- 71. The sacral plexus is formed by spinal nerves from L4, L5, and S1-S4. It gives rise to the sciatic nerve , which is actually composed of two nerves: the tibial nerve and the common fibular (common peroneal) nerve.
- 72. The sacral plexus gives rise to two principal nerves: the tibial nerve and the common fibular (peroneal) nerve. The sciatic nerve is composed of these two nerves wrapped in a common connective sheath. These two nerves separate just above the popliteal fossa.
- 73. The sciatic nerve splits into its separate components [tibial nerve and common fibular (peroneal) nerve] just superior to the popliteal fossa.
- 74. A tight piriformis muscle can compress the sciatic nerve
- 75. Don’t stick needles in the sciatic nerve!
- 76. The tibial nerve innervates the hamstrings, the gastrocnemius, the soleus, and several other muscles. It receives sensory input from the skin on the plantar surface of the foot.
- 77. The common fibular nerve (common peroneal nerve) innervates the peroneus (fibularis) longus, the tibialis anterior , and several other muscles of the leg and foot. This is the branch of the sciatic nerve that caused me problems! It receives sensory input from the anterolateral part of the leg, the toes, and dorsum of the foot.
- 78. Read about sacral plexus injuries and sciatica in the clinical view in your text.
- 79. Reflexes are rapid, automatic, involuntary reactions of muscles or glands to a stimulus
- 80. An example occurs when you accidentally touch a hot object. You remove your hand even before you are completely aware of the heat. A reflex can precede sensation (a reflex does not need to involve the brain)
- 81. A typical reflex arc
- 82. Generally, there are five steps involved in a neural reflex : stimulus, transmission via a sensory neuron, processing in CNS, transmission via a motor neuron, and an effector (muscle or gland) responds.
- 83. Read in your text about different types of reflexes for your own information if you desire.
- 84. The cranial (superior) portion of the neural tube expands and develops into the brain, while the caudal (inferior) part of the neural tube forms the spinal cord. The hollow neural canal develops into the central canal of the spinal cord. Neural tube
- 85. The bony vertebral column (dark line shown) grows faster than the spinal cord . A newborn’s spinal cord extends to about the level of L 3 . A child’s spinal cord may extend to the level of L 2 . An adult’s spinal cord typically terminates at the level of L 1 . Bony vertebral column
- 86. The inner delicate spinal cord terminates in an adult, as the conus medullaris, at the level of the L 1 vertebra.
- 87. Damage to the spinal cord can lead to paralysis or death
- 88. Severing the spinal cord above C3 typically leads to death by asphyxiation because the victim cannot use the spinal nerves to contract the intercostal muscles and cannot utilize the phrenic nerve to contract the diaphragm.
- 89. Christopher Reeve as Superman
- 90. In his fall, he crushed both the atlas (C1) and the axis (C2). He would have died by asphyxiation, but his accident was witnessed and rescue breathing was done. He became a very famous respirator-dependent quadriplegic .
- 91. Christopher Reeve after his fall.
- 92. Christopher Reeeve shortly before his death from an infected bed sore (decubitus ulcer). He did a great deal to advance research on spinal trauma.
- 94. Damage below C3 also results in quadriplegia , but the person can still utilize their diaphragm for breathing via their intact phrenic nerves .
- 97. WHICH OF THE FOLLOWING IS CORRECT ? A “FOOT DROP” IS TYPICALLY CAUSED BY DAMAGE TO THE COMMON PERONEAL NERVE B THE OBTURATOR NERVE STIMULATES ADDUCTION OF THE THIGH C THE EMBRYONIC NEURAL CANAL BECOMES THE CENTRAL CANAL OF THE SPINAL CORD D THE PHRENIC NERVE IS FUNCTIONAL FOLLOWING TRANSECTIONS OF THE SPINAL CORD AT C 5 /C 6 E ALL OF THE ABOVE