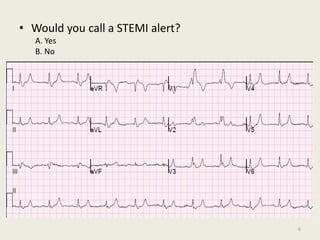
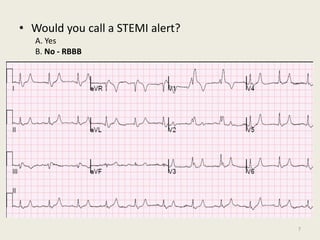
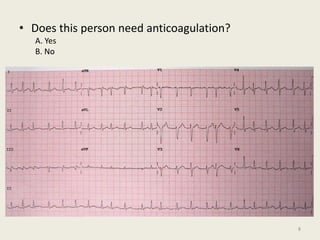
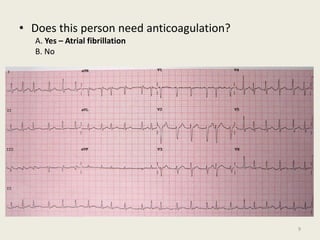
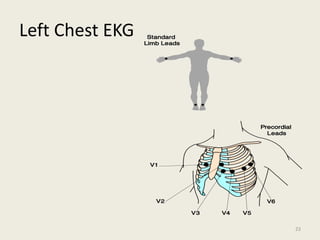
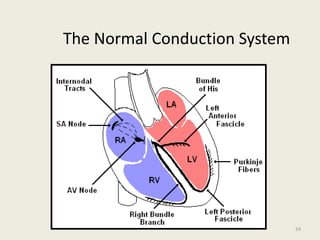
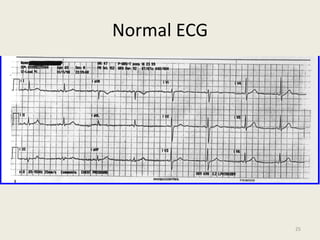
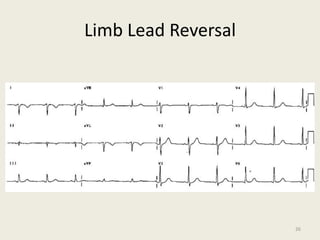
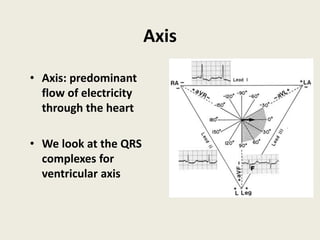
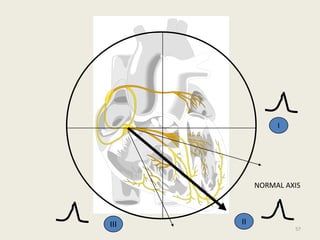
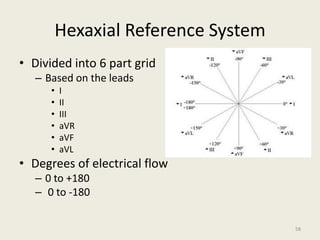
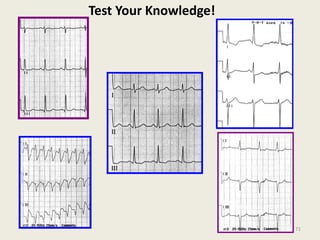
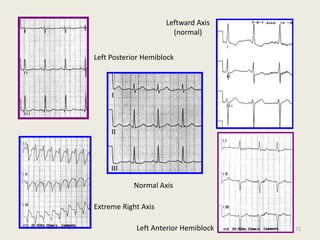
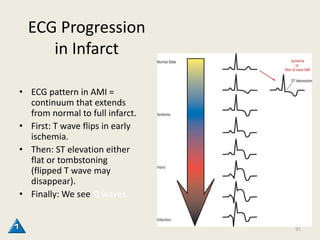
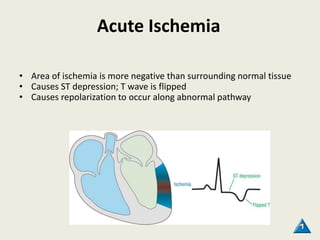
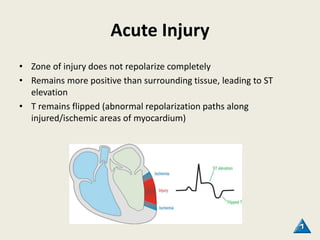
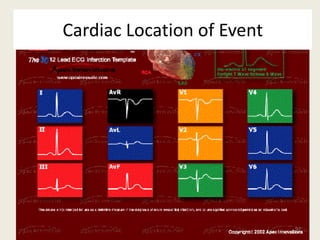
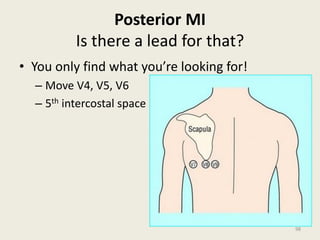
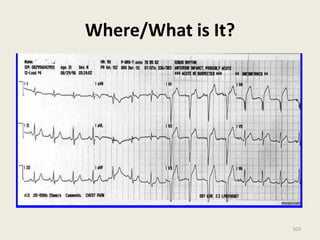
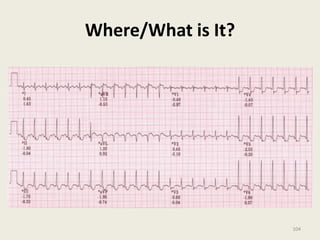
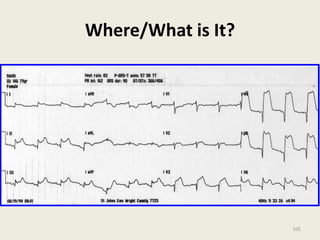
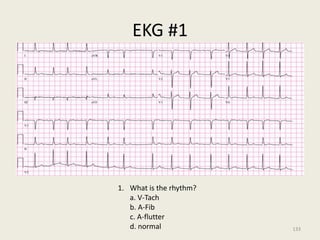
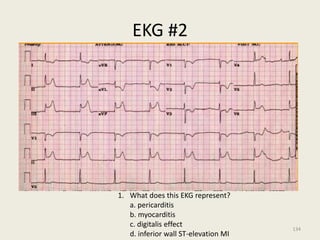
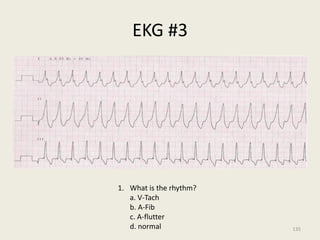
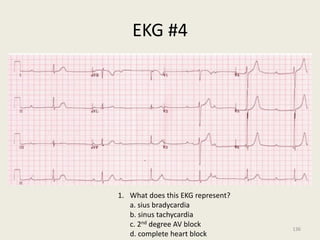
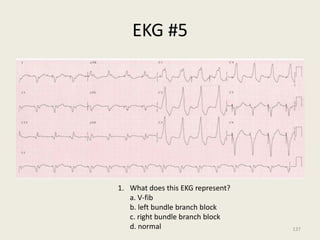
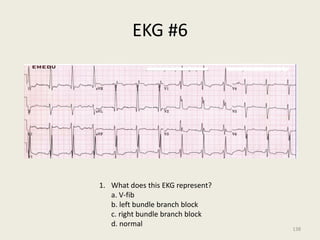
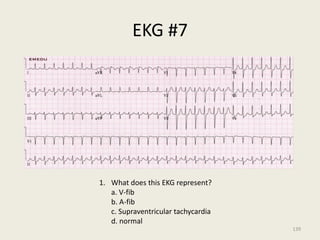
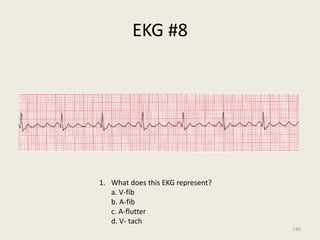
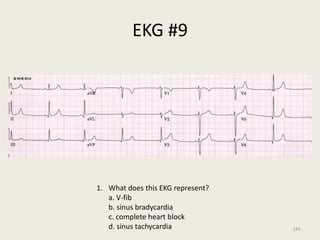
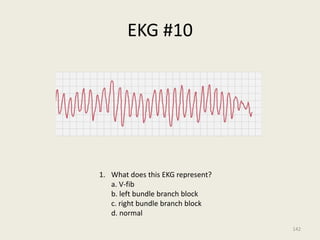
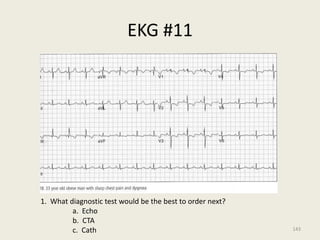
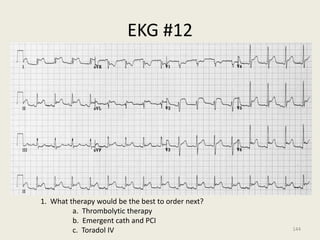
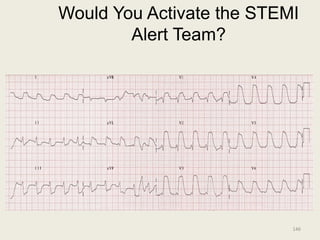
The document discusses a presentation on interpreting 12-lead electrocardiograms (EKGs). It covers proper lead placement, identifying normal EKG intervals and rhythms, recognizing conduction blocks and bundle branch blocks, determining heart axis, and interpreting signs of ischemia including ST elevation myocardial infarctions (STEMIs). The objectives are to learn EKG interpretation skills like identifying arrhythmias, conduction abnormalities, axis deviations, and using ST segment changes to localize infarct location.