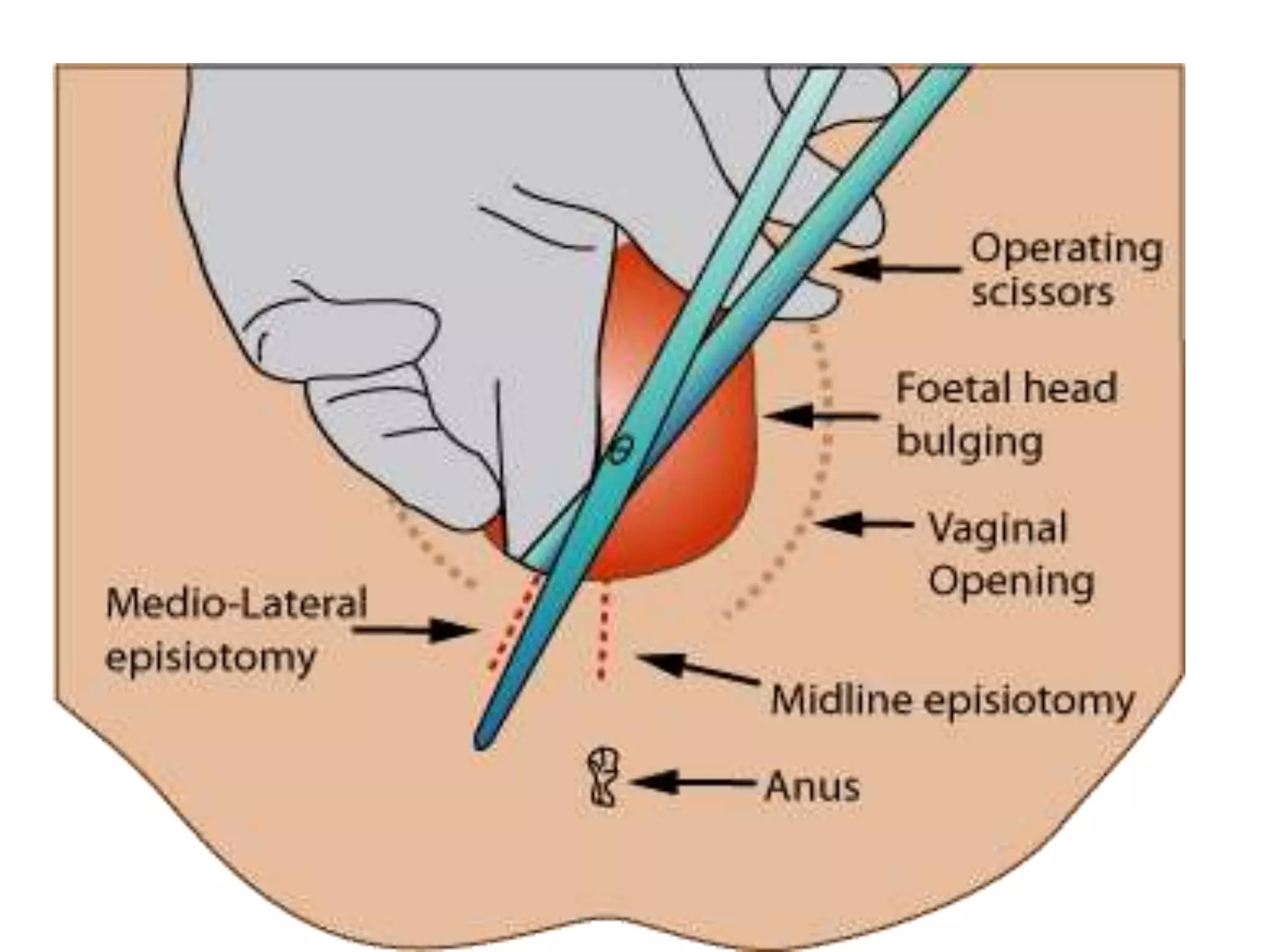
This document discusses episiotomies and perineal tears that can occur during childbirth. It defines an episiotomy as a surgically planned incision made in the perineum and posterior vaginal wall during the second stage of labor. It notes that routine episiotomies are no longer commonly performed and discusses the types of episiotomies including midline and mediolateral, along with their risks and benefits. Perineal tears are also defined as tears between the vagina and rectum that can range in severity from first to fourth degree. Risk factors, complications, classification, management, and prevention of perineal tears are outlined.