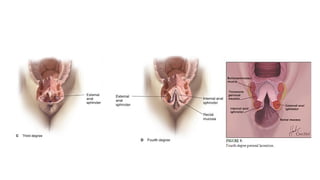
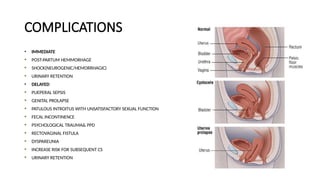
Perineal tears are common injuries during vaginal childbirth, particularly affecting primigravida women, and can result in various complications, including persistent symptoms post-delivery. The degree of tear classifications (1st to 4th degree) is critical for management, with surgical repair advised for more severe injuries, especially 3rd and 4th degree ones. Preventative measures during labor and careful monitoring, alongside clear documentation and counseling, are essential for improving outcomes and minimizing legal repercussions.