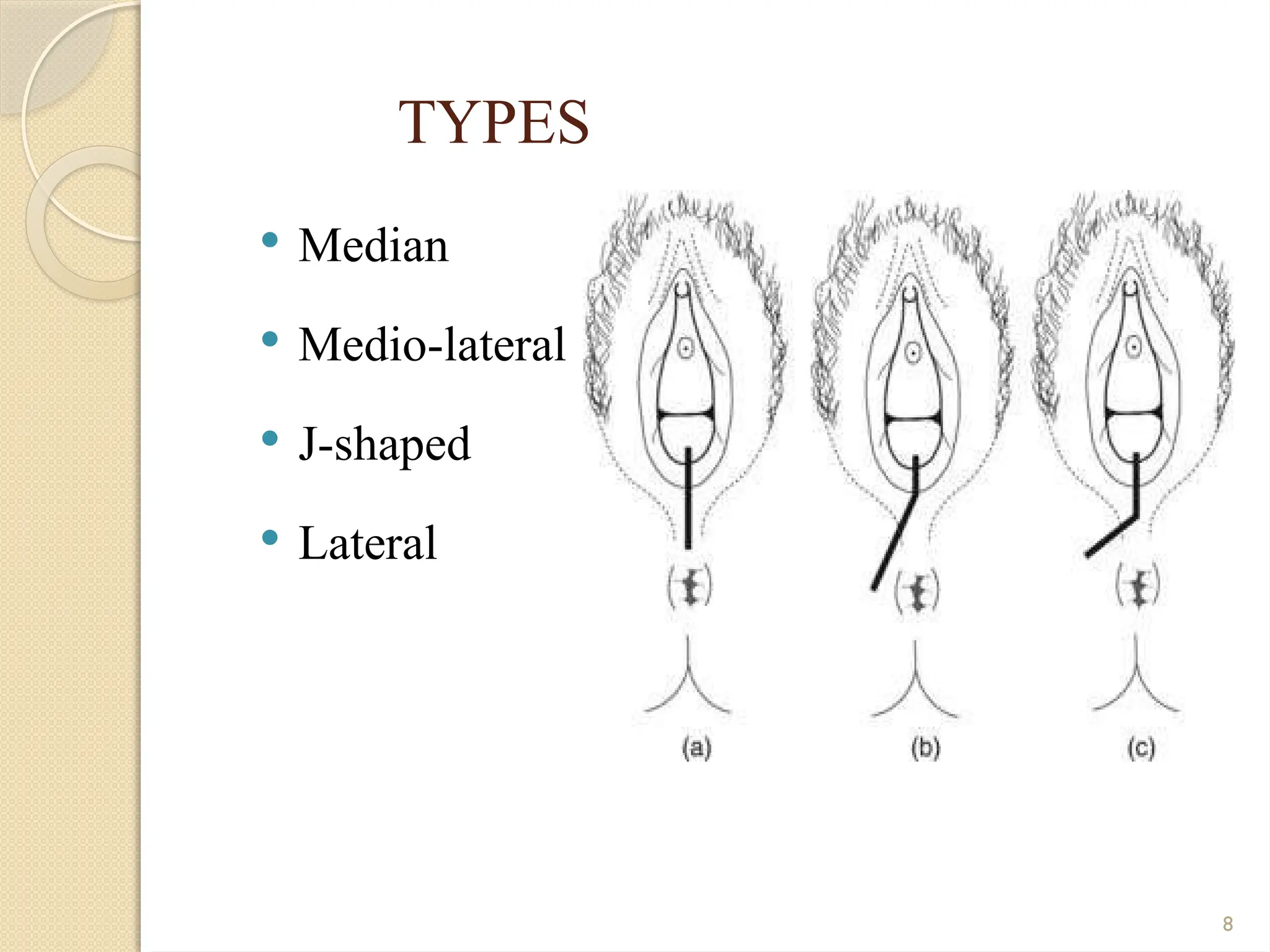
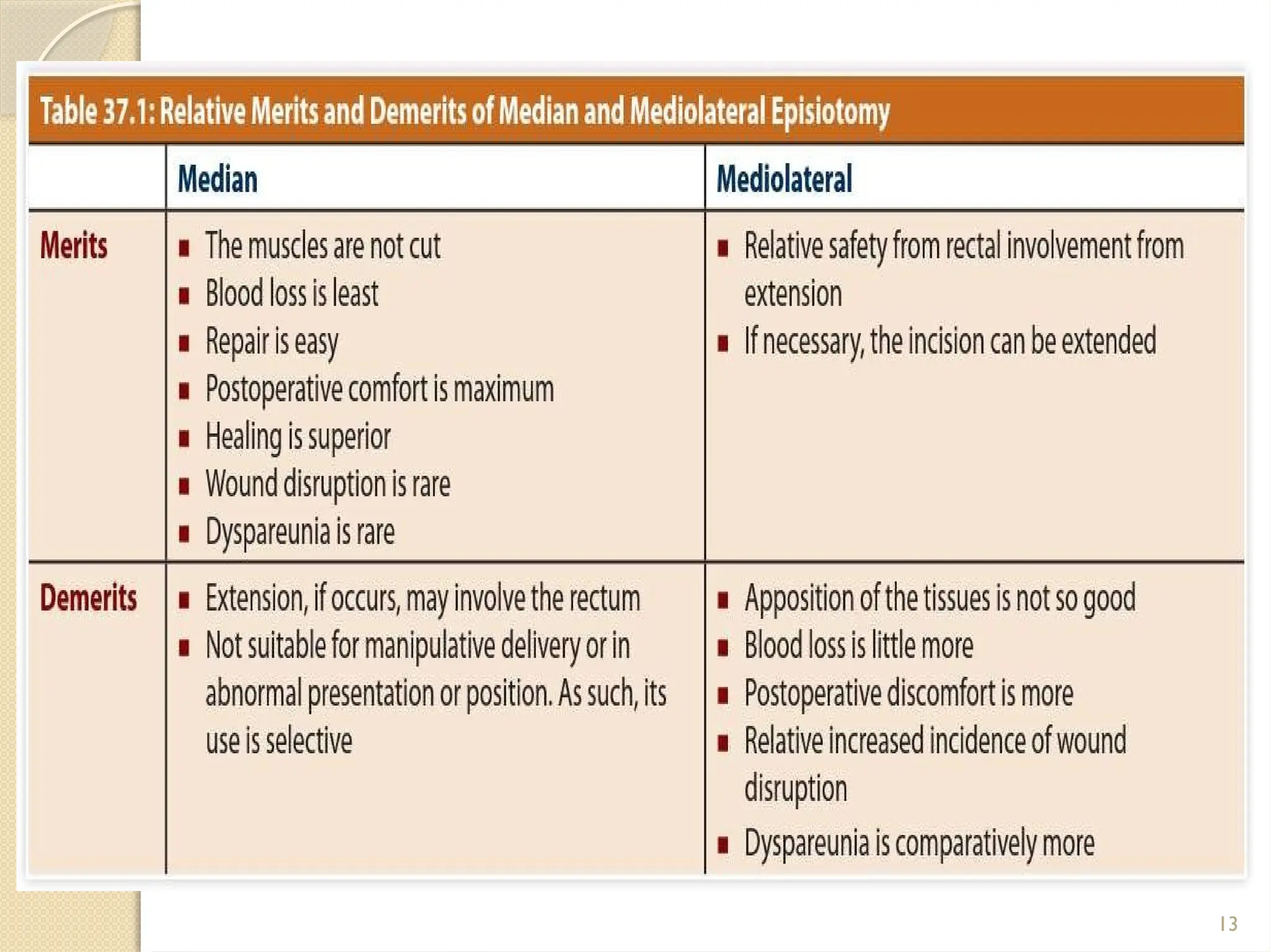
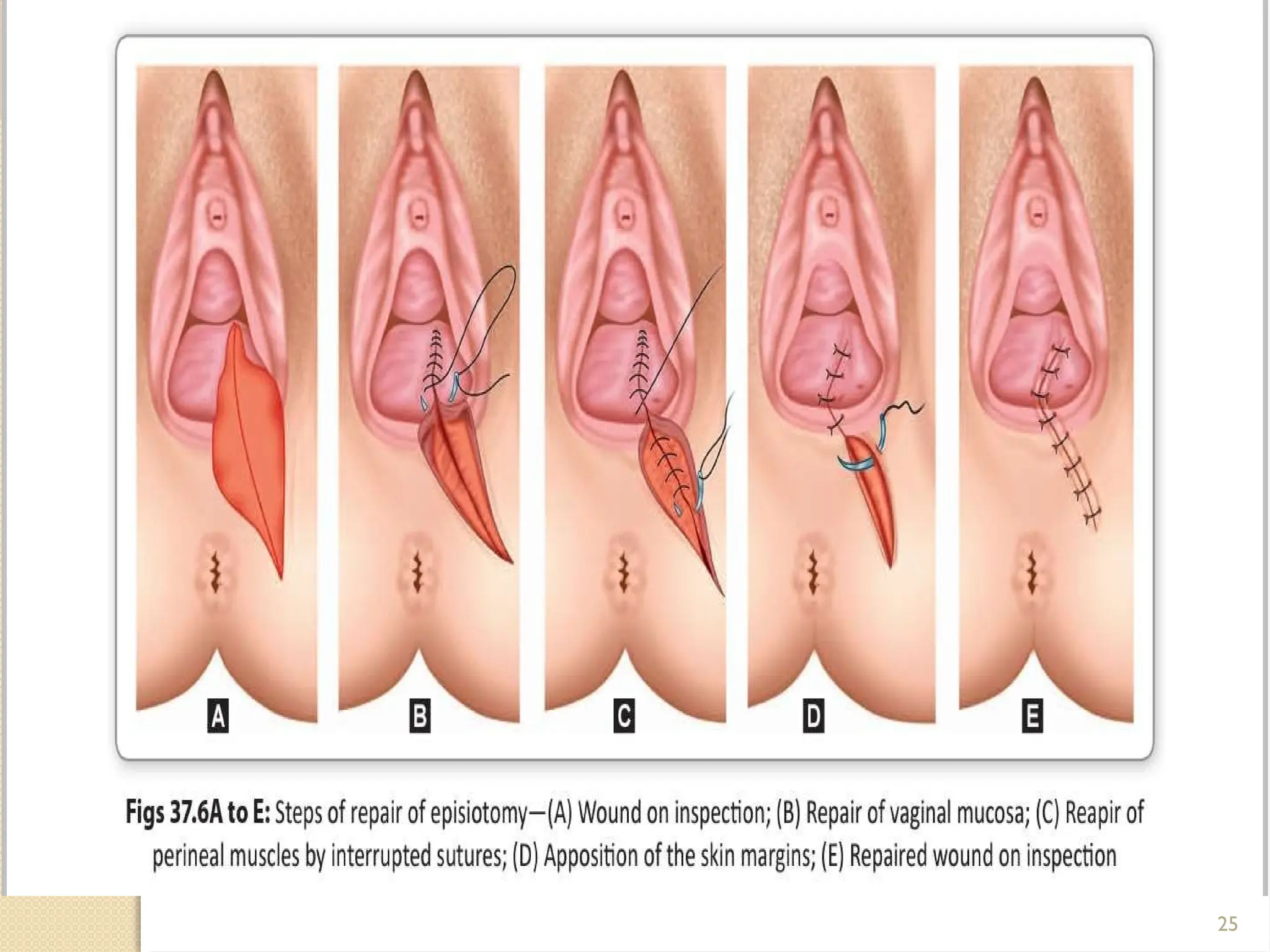
The document provides a comprehensive overview of episiotomy and perineal tears during childbirth, including definitions, indications, types, and complications of these procedures. It outlines various surgical techniques for episiotomy, emphasizing the advantages and disadvantages of each type, along with postoperative care and potential complications. Additionally, it describes perineal tears, their classifications, and management strategies, highlighting the importance of addressing them properly to ensure maternal health.