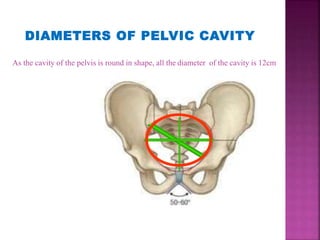
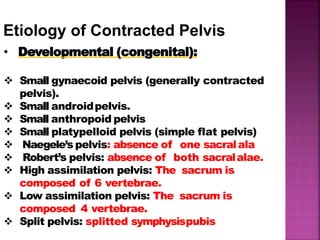
The document discusses the pelvis and cephalopelvic disproportion (CPD). It defines the false pelvis and true pelvis, and lists the normal diameters of the pelvic inlet, cavity, and outlet. It describes a contracted pelvis as having one or more diameters reduced by 1 cm or more below normal. Causes of a contracted pelvis include developmental factors, trauma, infections, tumors, and metabolic bone diseases. Degrees of CPD range from minor to extreme. Management depends on the degree of disproportion and may include a trial of vaginal delivery, cesarean section, or craniotomy. Complications can affect both mother and fetus.