Download as PDF, PPTX
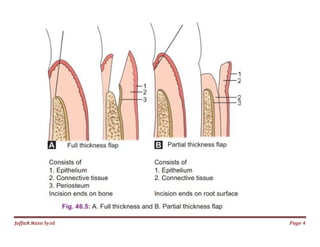
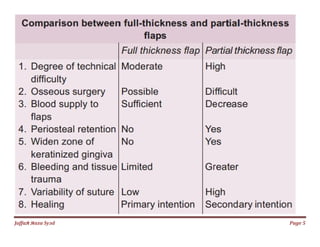


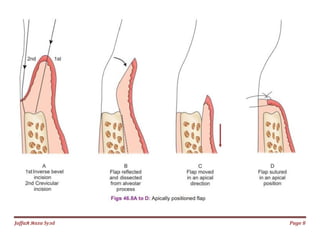
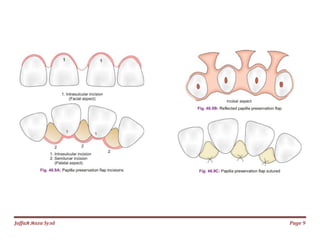
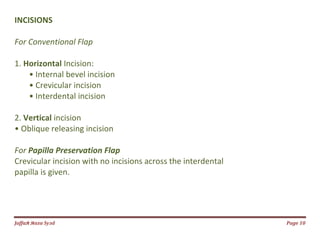

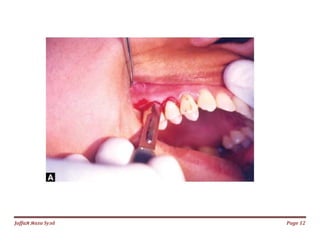
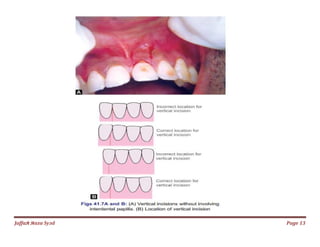
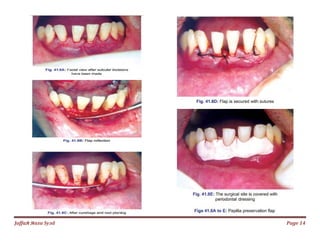

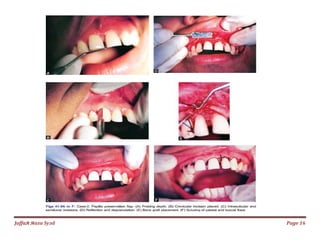

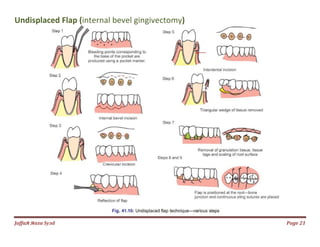

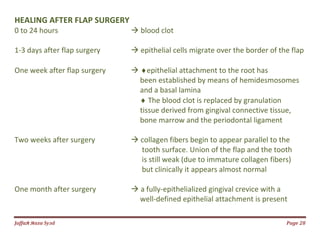

A periodontal flap is a section of gingiva and/or mucosa surgically elevated to provide access to the bone and root surfaces. There are several types of flaps classified by thickness, management of papilla, and placement after surgery. The basic requirements are that the base and size allow for adequate blood supply and exposure of underlying defects without damaging vessels or nerves. Incisions for conventional and papilla preservation flaps are also described. Healing takes several weeks as the blood clot is replaced by granulation tissue and collagen fibers form to reattach the gingiva.























































































