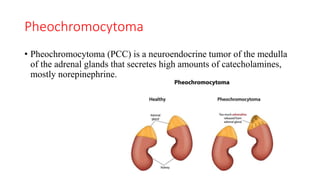
Downloaded 59 times
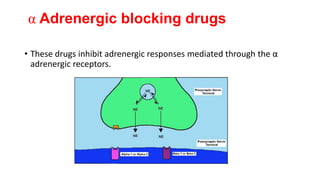
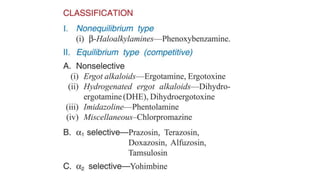
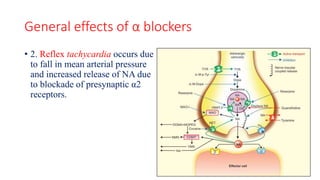
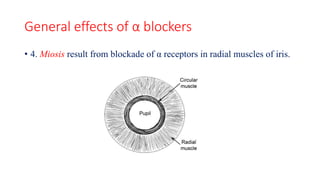
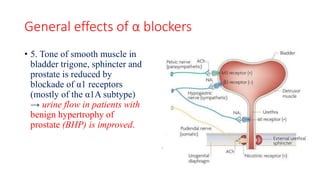
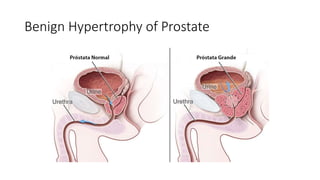
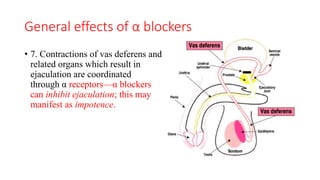

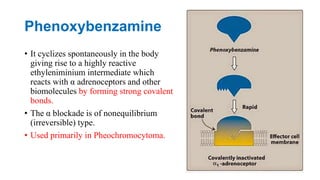


α blockers work by inhibiting adrenergic responses mediated through α adrenergic receptors. They reduce peripheral resistance and blood pressure by blocking vasoconstrictor α1 receptors. Common side effects include reflex tachycardia, nasal stuffiness, miosis, and reduced ejaculation. Phenoxybenzamine is irreversibly binds to receptors. Prazosin is highly selective for α1 receptors. It is used to treat hypertension and benign prostatic hyperplasia. Tamsulosin is relatively selective for α1A/α1D receptors in the bladder and prostate and causes fewer side effects than non-selective α blockers. α blockers are used to treat pheochromocytoma,
















































































