Downloaded 65 times


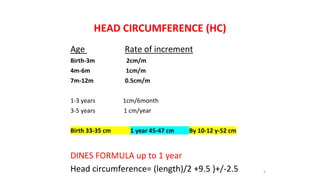




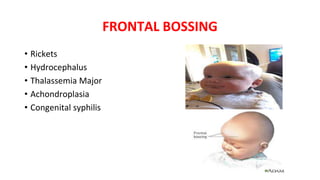
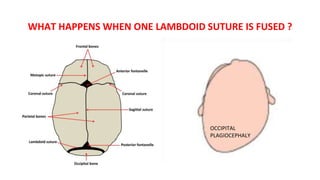

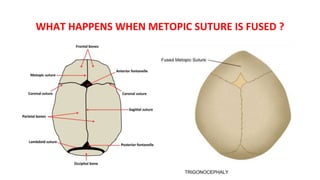
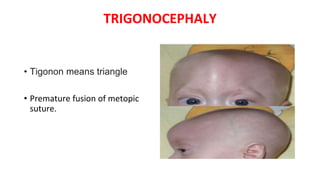
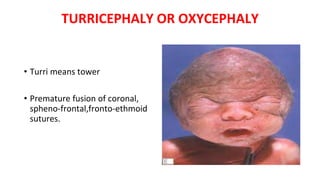
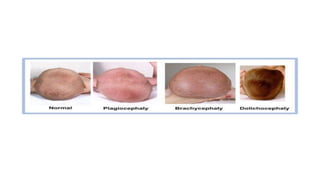
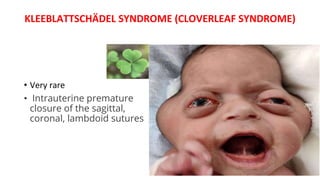
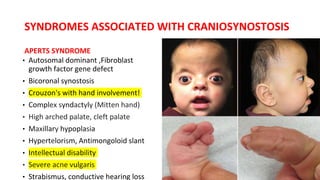


This document discusses disorders of head and teeth growth. It provides details on measuring head circumference and normal growth rates. Microcephaly is defined as a head circumference more than 3 standard deviations below the mean. Causes of primary microcephaly include familial, genetic diseases, structural brain abnormalities, and craniosynostosis. Secondary microcephaly results from insults affecting brain growth and has causes such as maternal infections/diseases, perinatal brain injuries, and postnatal illnesses. Macrocephaly is a head circumference over 2 standard deviations above the mean and can be caused by abnormalities of the cranial vault, brain, CSF, or space occupying lesions. Craniosynostosis is premature fusion of cranial sut