




















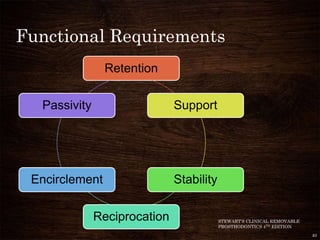









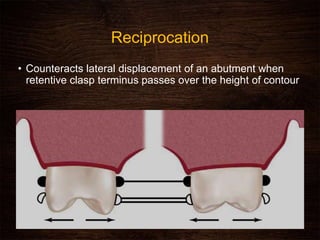







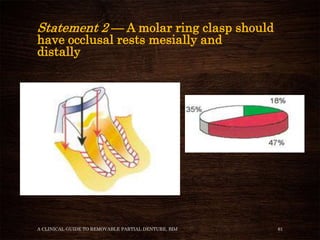


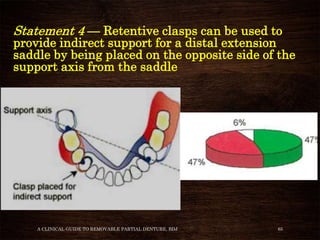




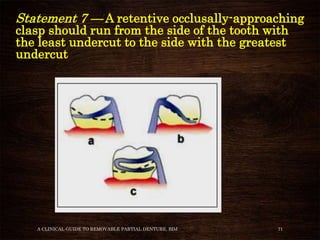














































The document discusses various aspects of clasp design for removable partial dentures. It begins by defining what a clasp is and describing different clasp classifications such as occlusally approaching and gingivally approaching clasps. It then examines specific clasp designs like circumferential, bar/Roach type, and combination clasps. The document outlines the functional requirements of clasps, including retention, support, stability, and reciprocation. It also reviews several statements about clasp design, discussing whether prosthodontic experts agree or disagree with them based on clinical factors.





















































































