Downloaded 311 times




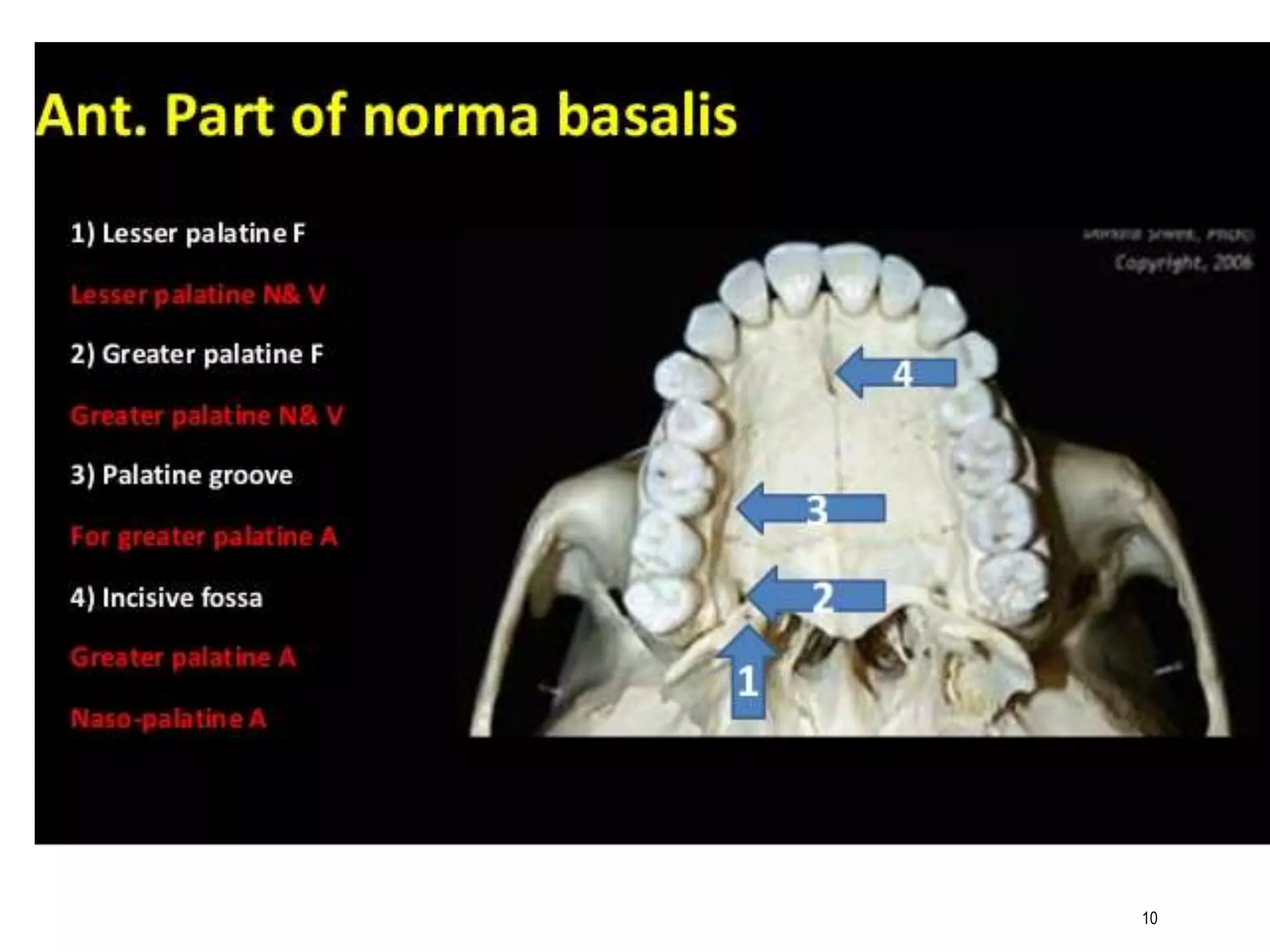
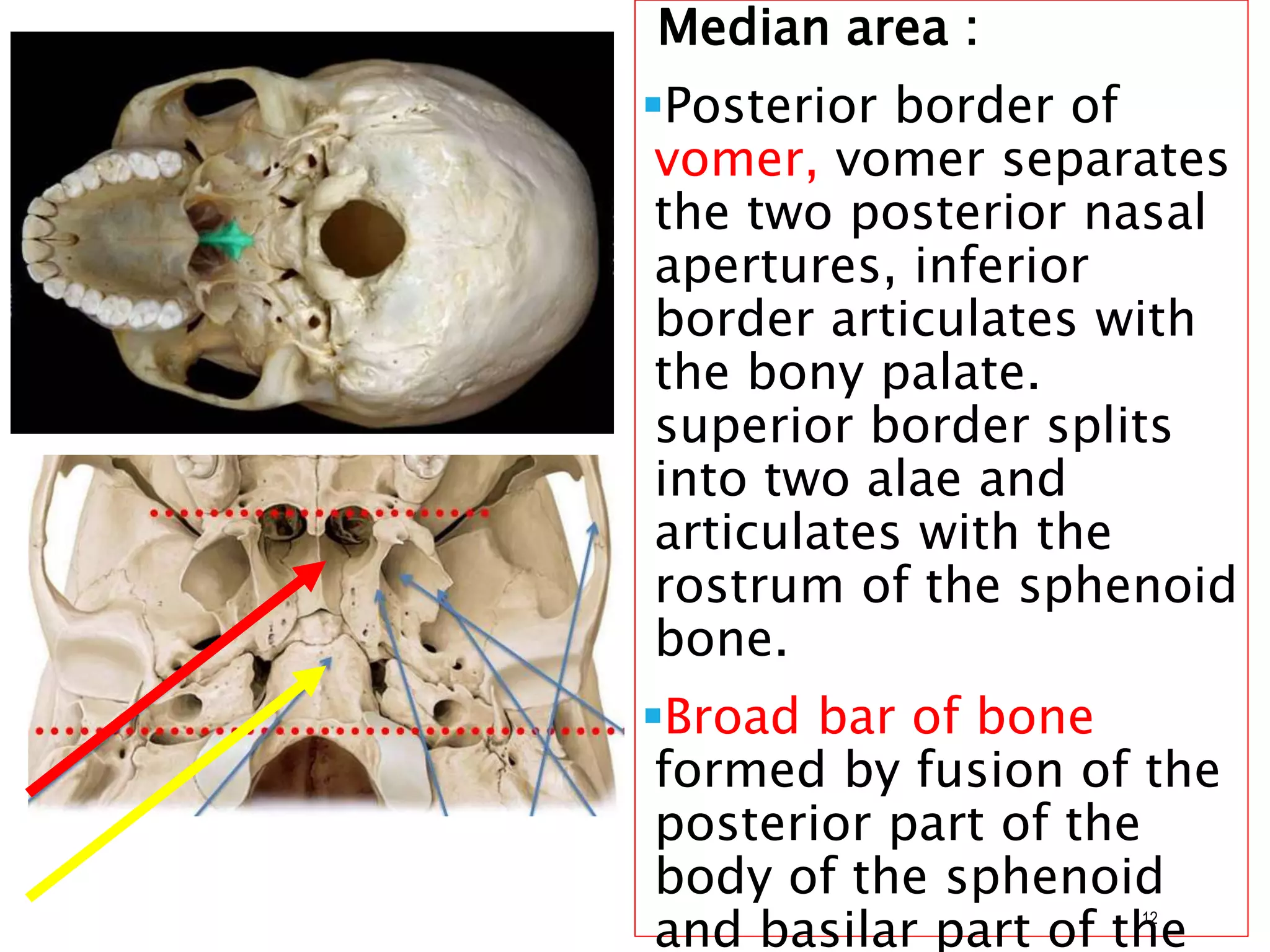

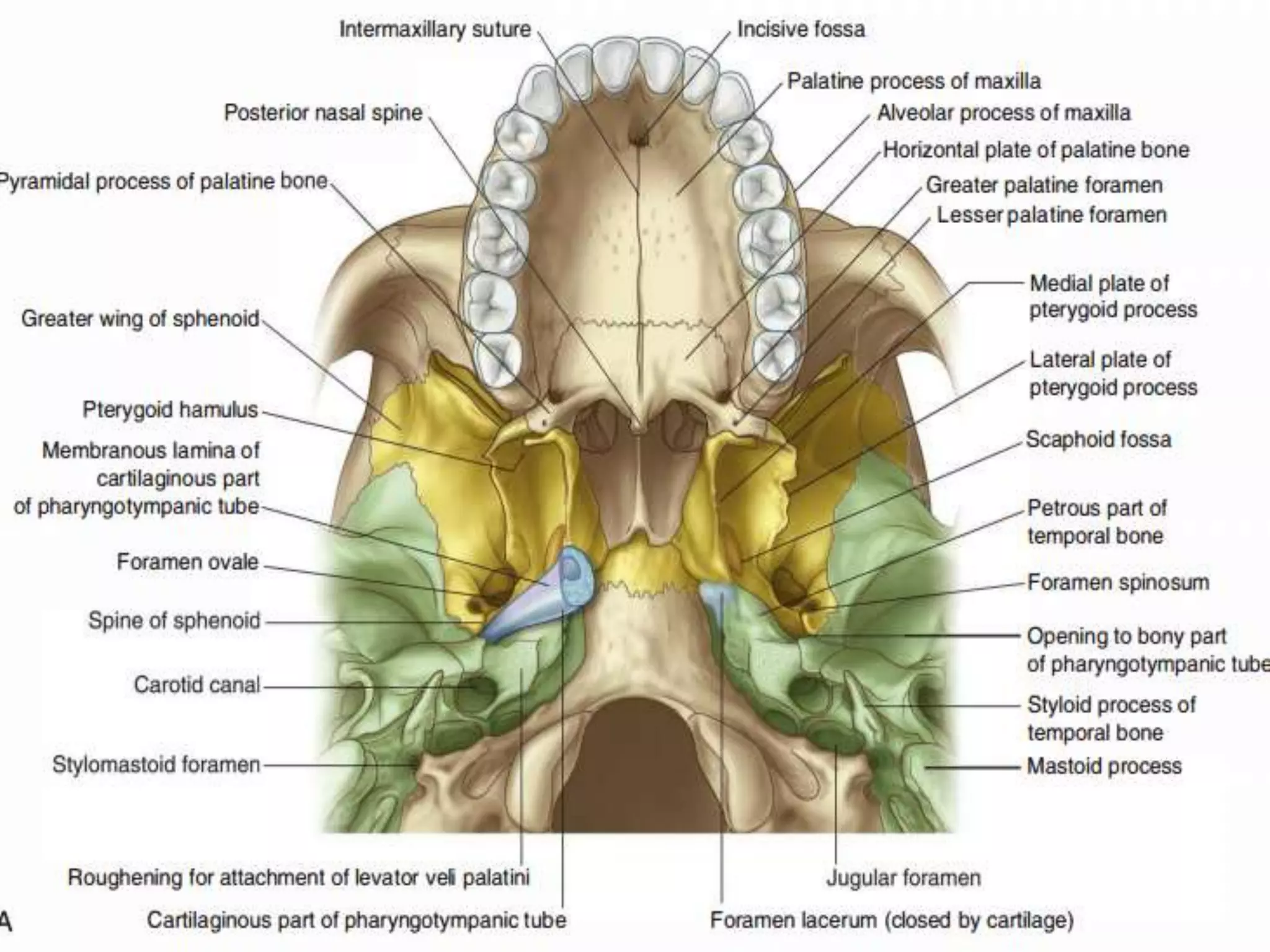
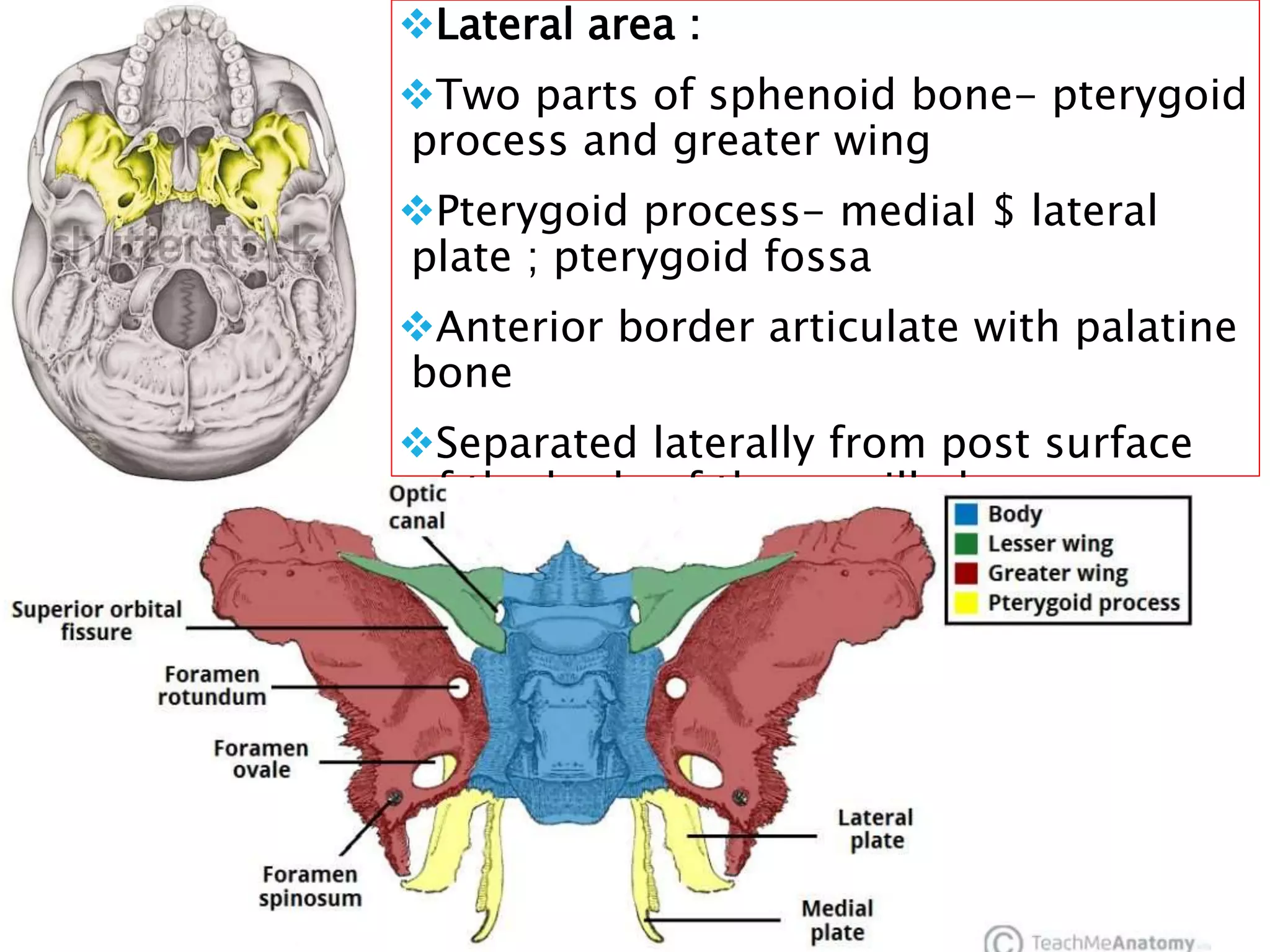

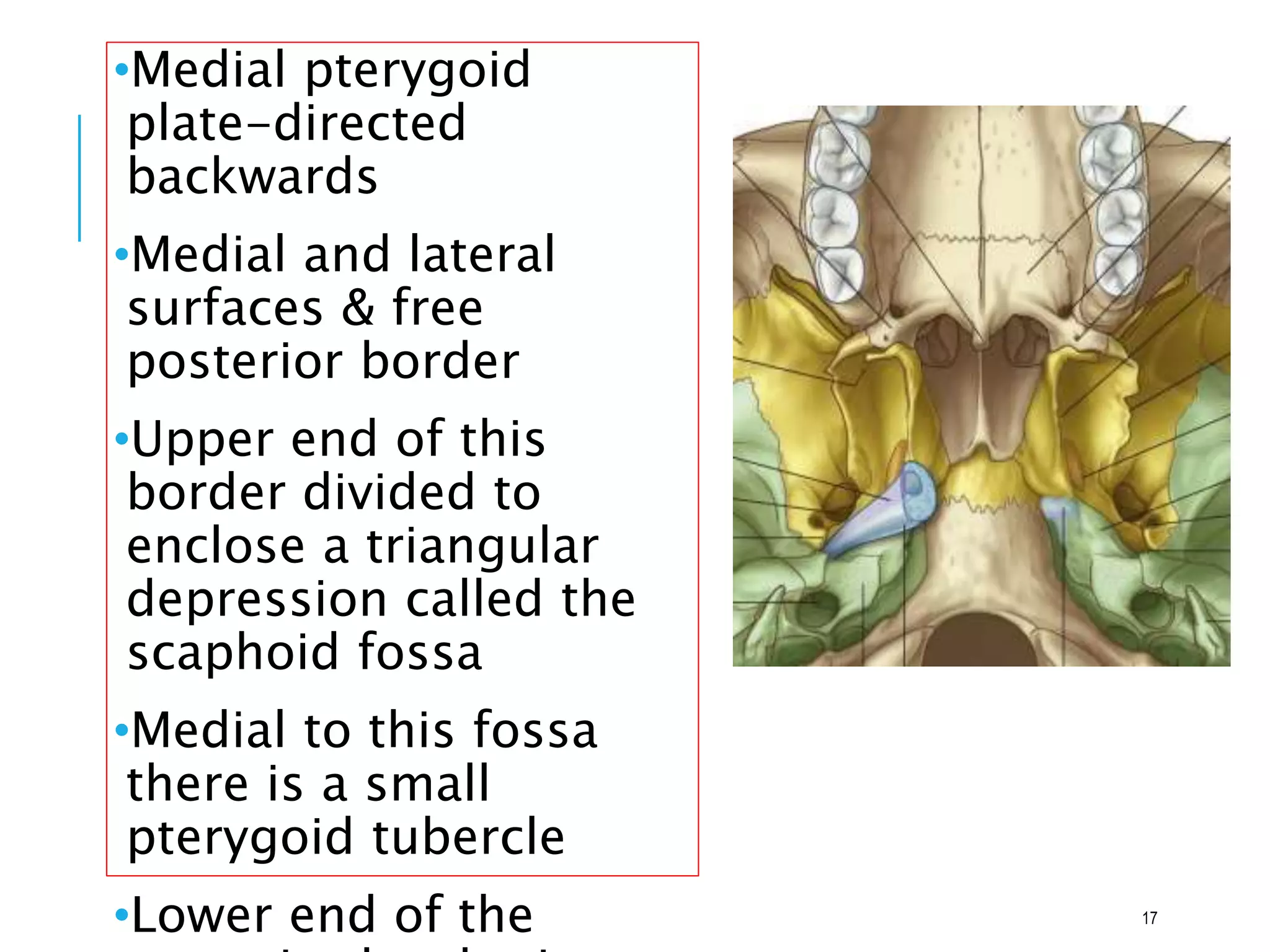




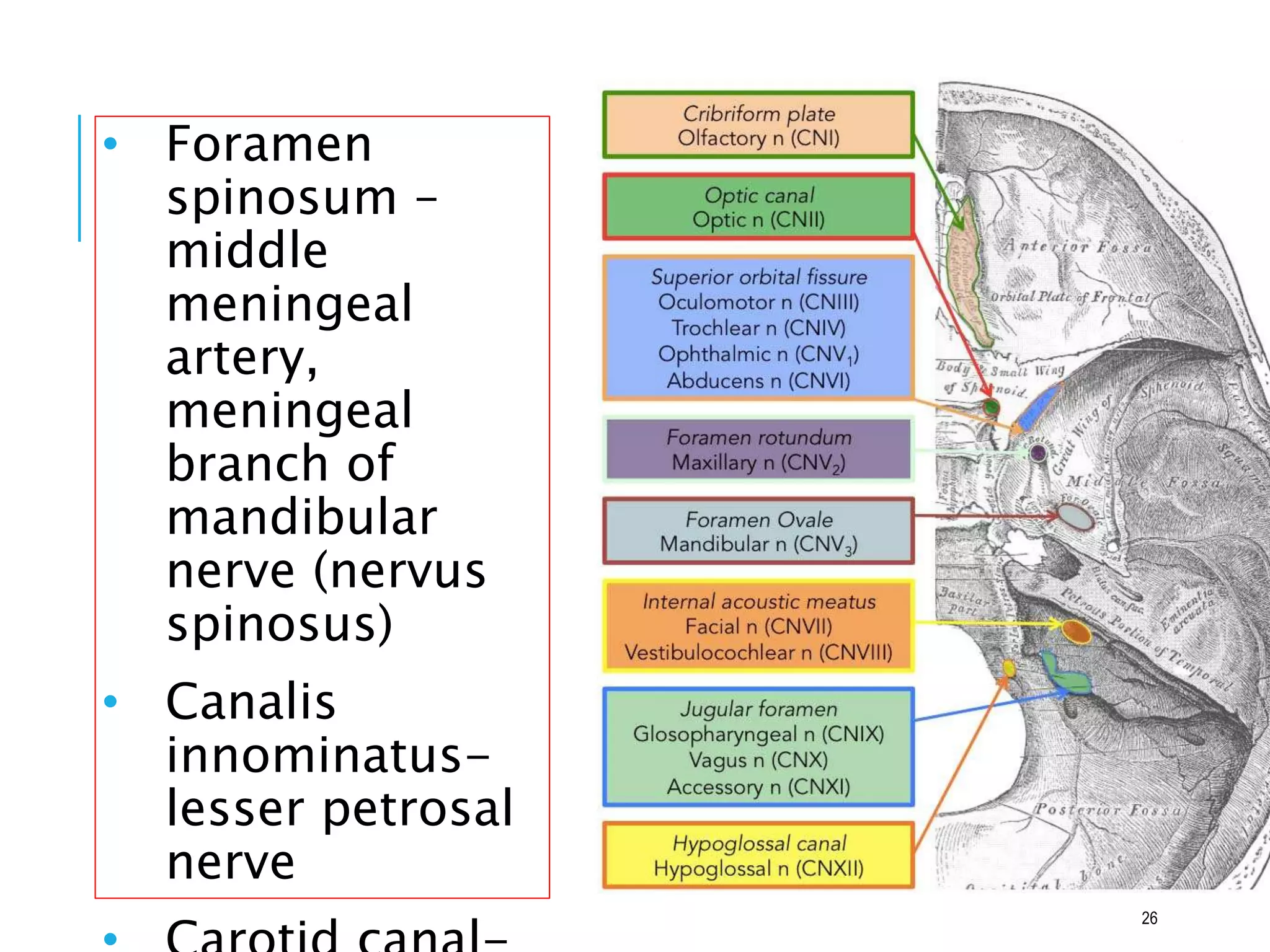

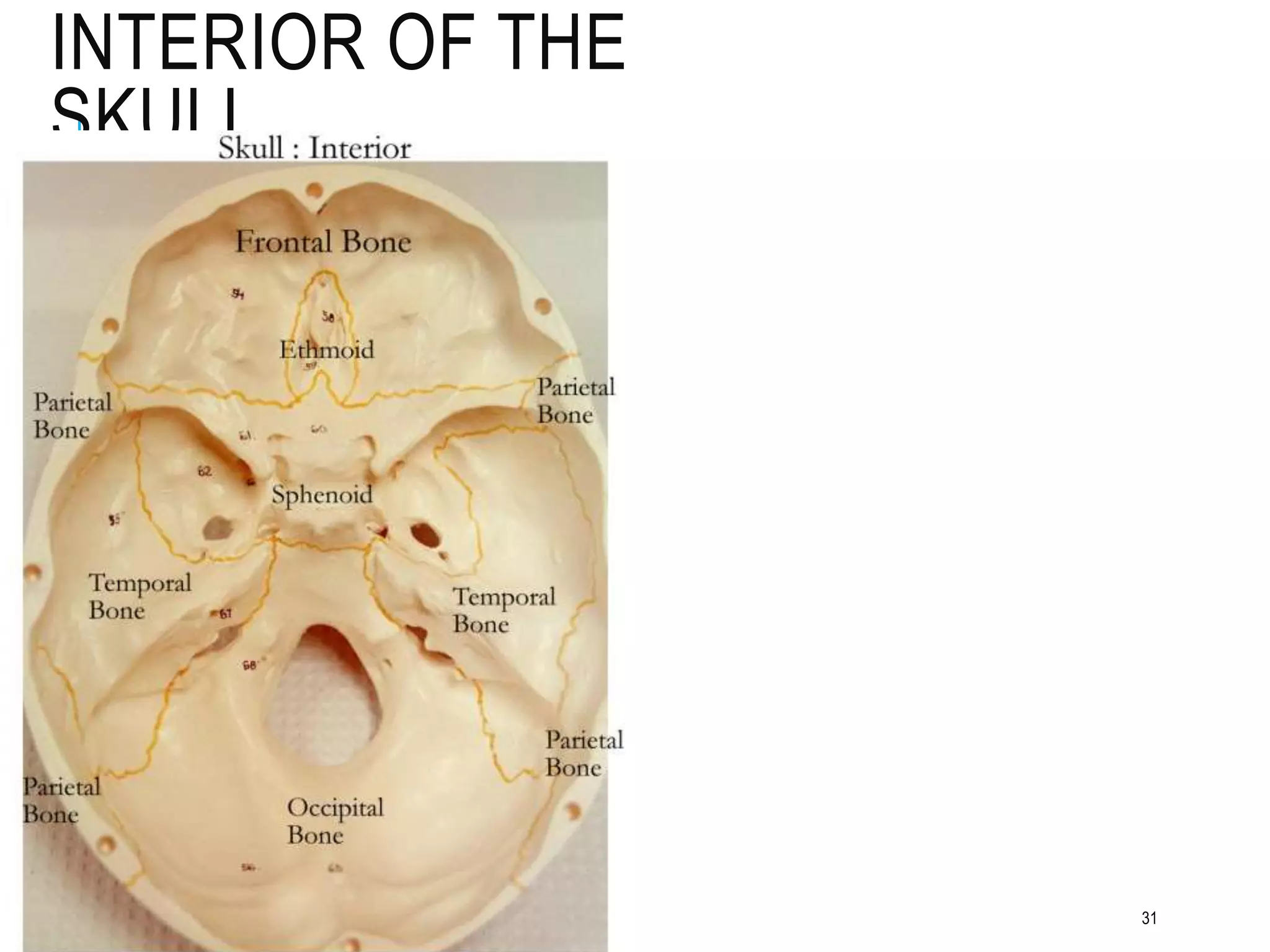
















1. The document describes the parts and structures of the norma basalis of the human skull. It is divided into anterior, middle, and posterior parts. 2. The anterior part contains the alveolar arch, hard palate, incisive fossa, and palatine foramina. The middle part contains the median area with the vomer bone and lateral areas with the sphenoid and temporal bones. 3. The posterior part contains the foramen magnum and occipital bone laterally. Various structures like nerves and vessels pass through skull foramina.




























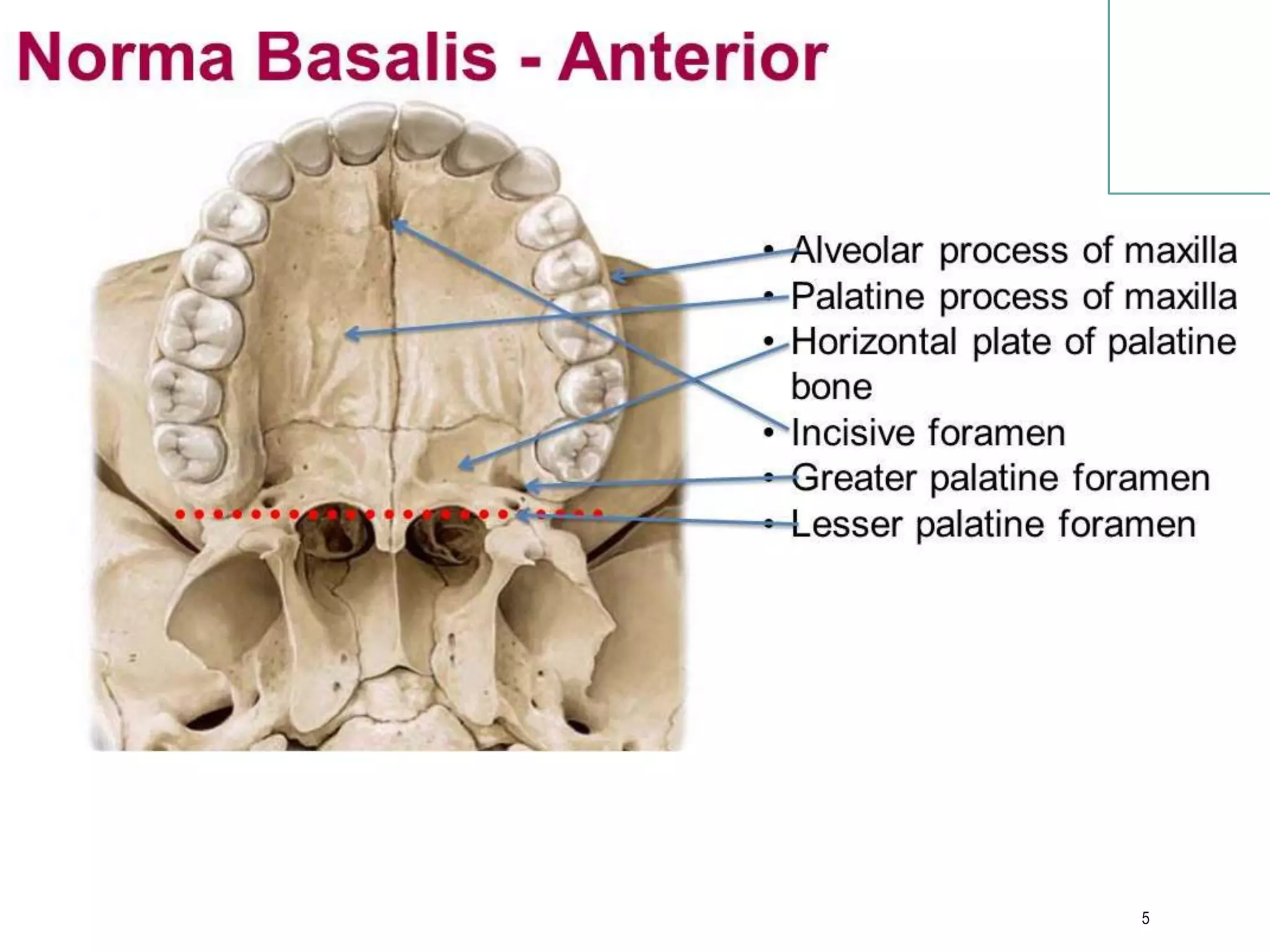
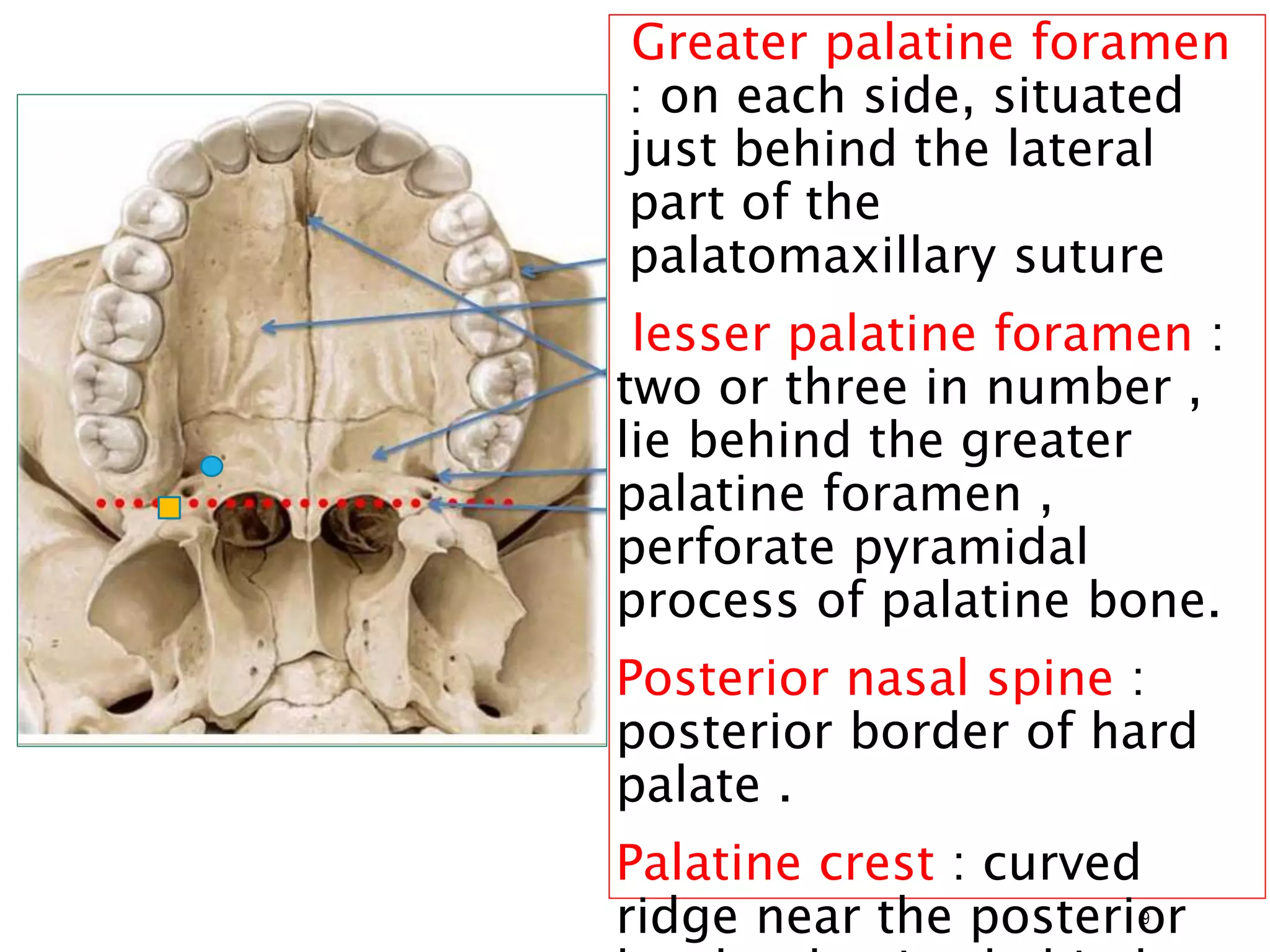
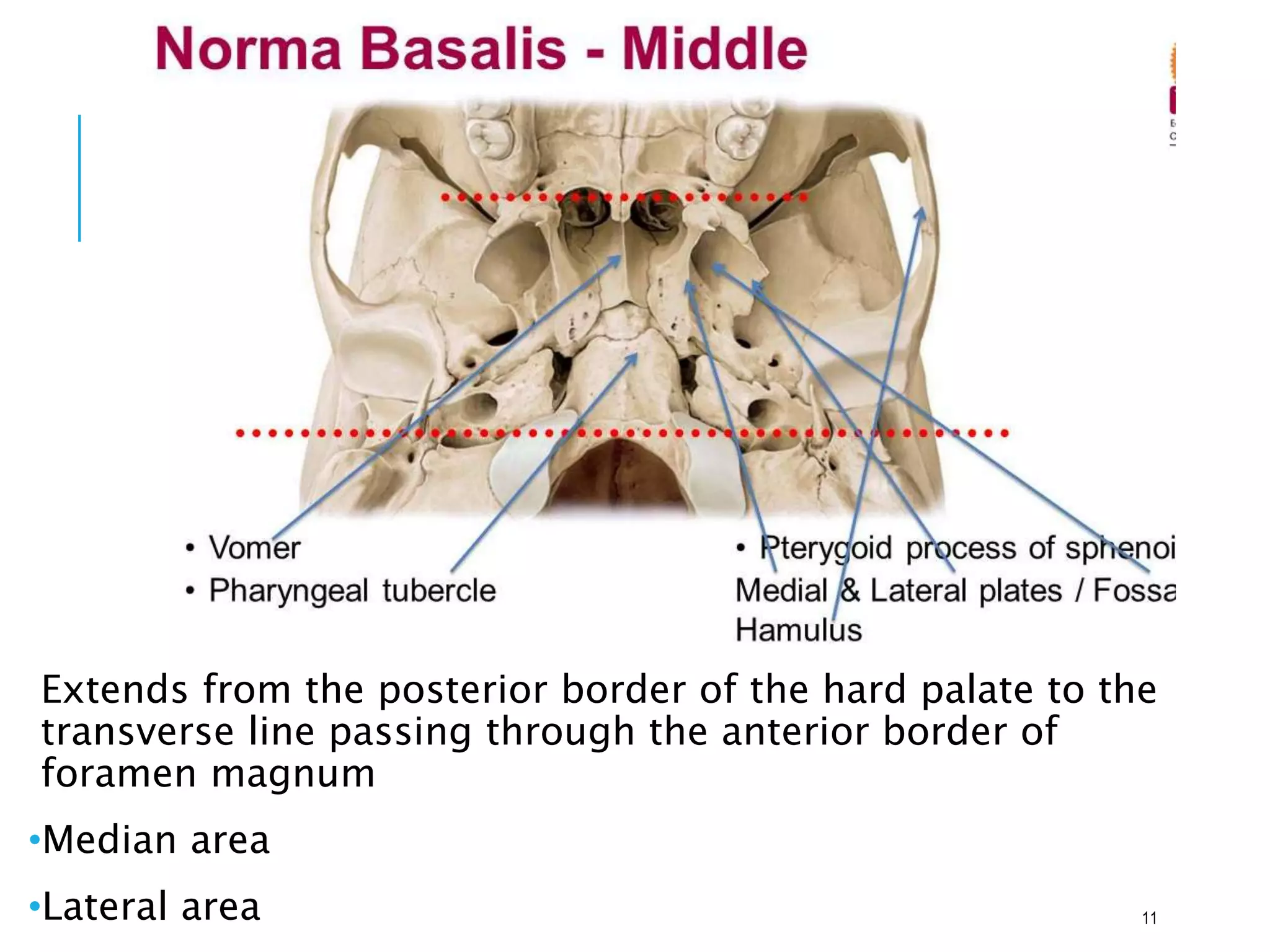
![Introduction to skull[1]](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontoskull1-170504174910-thumbnail.jpg?width=640&height=640&fit=bounds)