3
Chapter Outline
1. Roleof Direct Retainers
2. Basic Principles of Clasp Design
3. Types of Direct Retainers
4. Criteria for selecting a given Clasp design
5. Types of Clasp assemblies
6. Implants as Direct Retainers
7. Analysis of Tooth Contours for retentive clasps
8. Amount of Retention
9. Internal Attachments
10.Other types of Retainers
4.
Definition of Directretainers
•The component part which resist the movement away
from the teeth and/or tissue provides retention for
the prosthesis is called as the Direct retainers.
5.
Direct retainer’s rolein control of prosthesis
movement
• Provide Retention
• However it ability to resist displacement also depends on the
stability of the minor and major connectors, rest and tissue
bases. (hence all should be rigid)
• It resists dislodgment forces like forces from sticky food,
gravitational pull
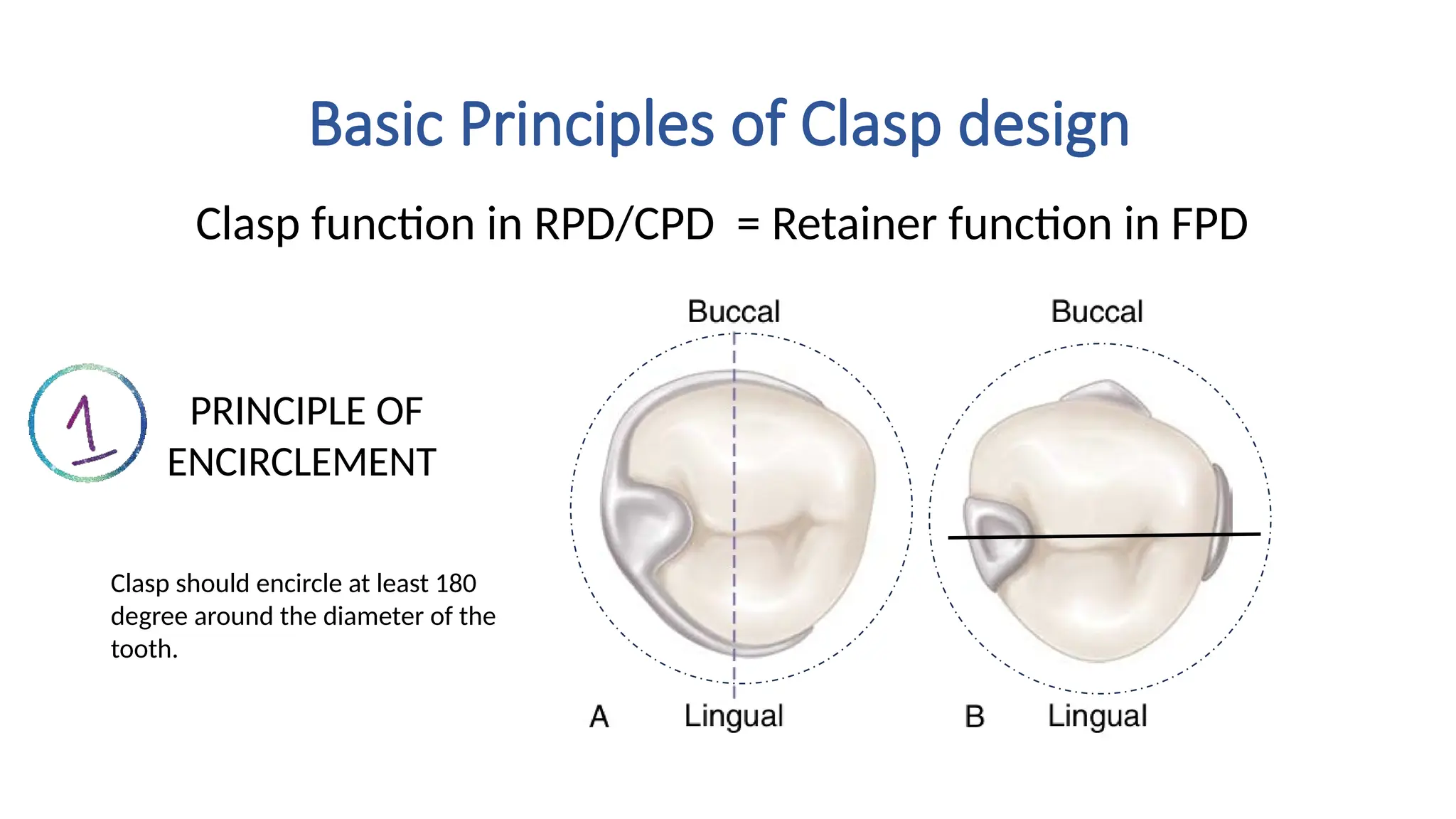
Basic Principles ofClasp design
Clasp function in RPD/CPD = Retainer function in FPD
PRINCIPLE OF
ENCIRCLEMENT
Clasp should encircle at least 180
degree around the diameter of the
tooth.
8.
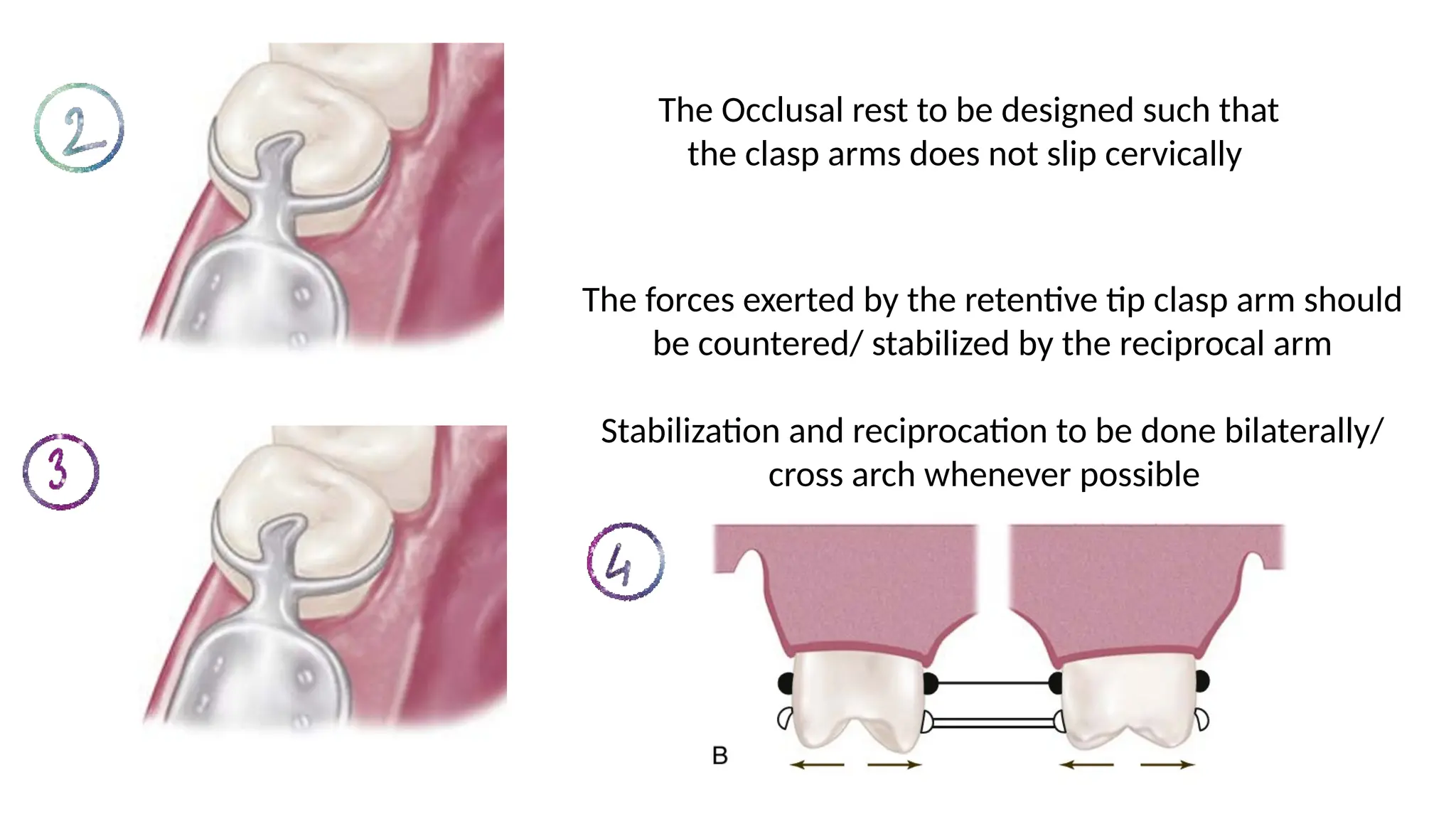
The Occlusal restto be designed such that
the clasp arms does not slip cervically
The forces exerted by the retentive tip clasp arm should
be countered/ stabilized by the reciprocal arm
Stabilization and reciprocation to be done bilaterally/
cross arch whenever possible
9.
The path ofplacement and path of
escapement of the clasp should be same and
parallel.
Retention forces should be minimum enough
to resist the dislodgment force
10.
Reciprocal arm function
Reciprocation:Resist the tipping
forces exerted by the retentive
clasp tip while placing and
removal of denture.
Cross arch Stabilization: Resist
horizontal movements of the
denture.
Indirect retainer: Lifting of distal extension denture
base can be prevented by the rigid reciprocal arm
11.
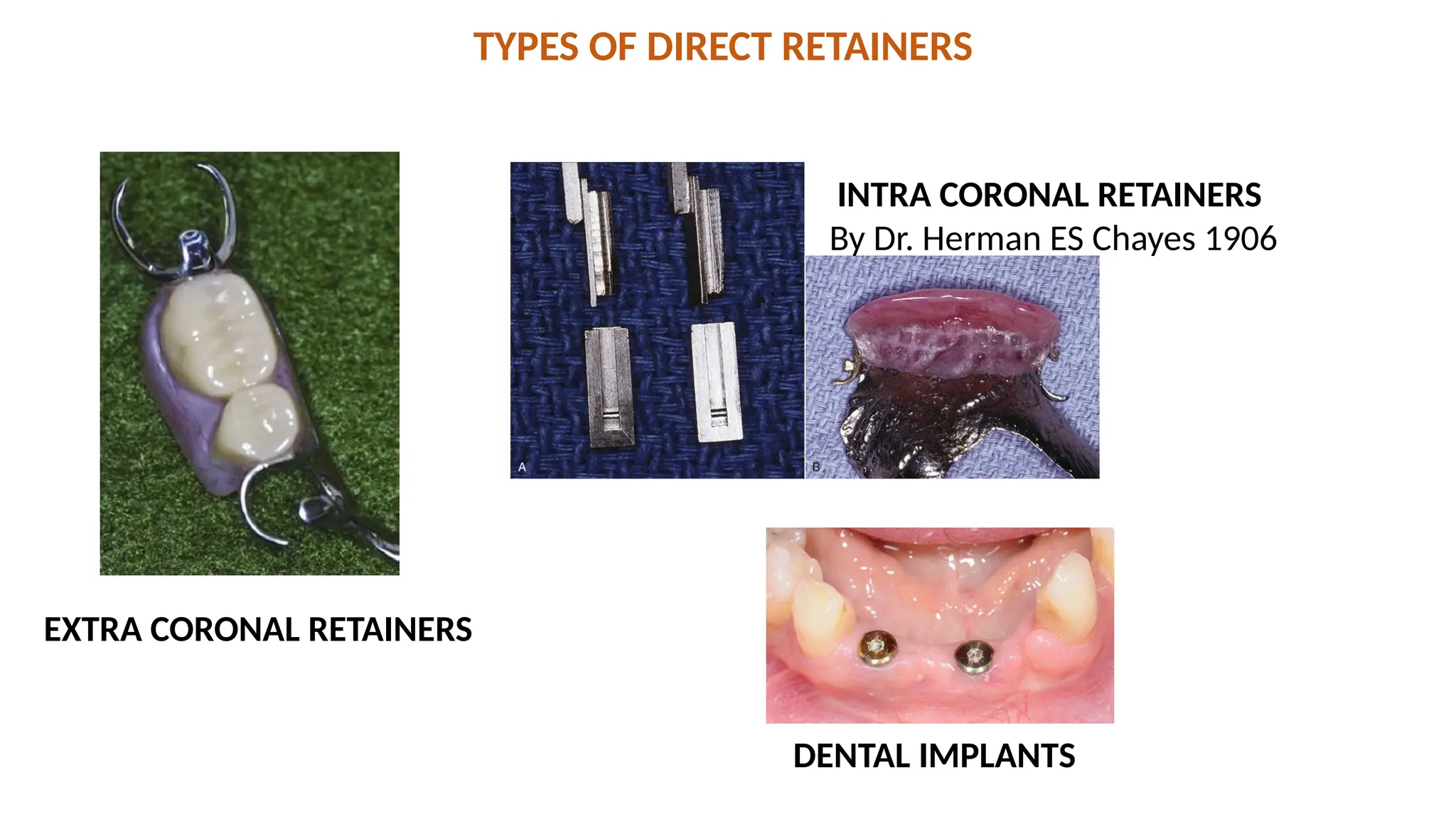
TYPES OF DIRECTRETAINERS
INTRA CORONAL RETAINERS
By Dr. Herman ES Chayes 1906
EXTRA CORONAL RETAINERS
DENTAL IMPLANTS
12.
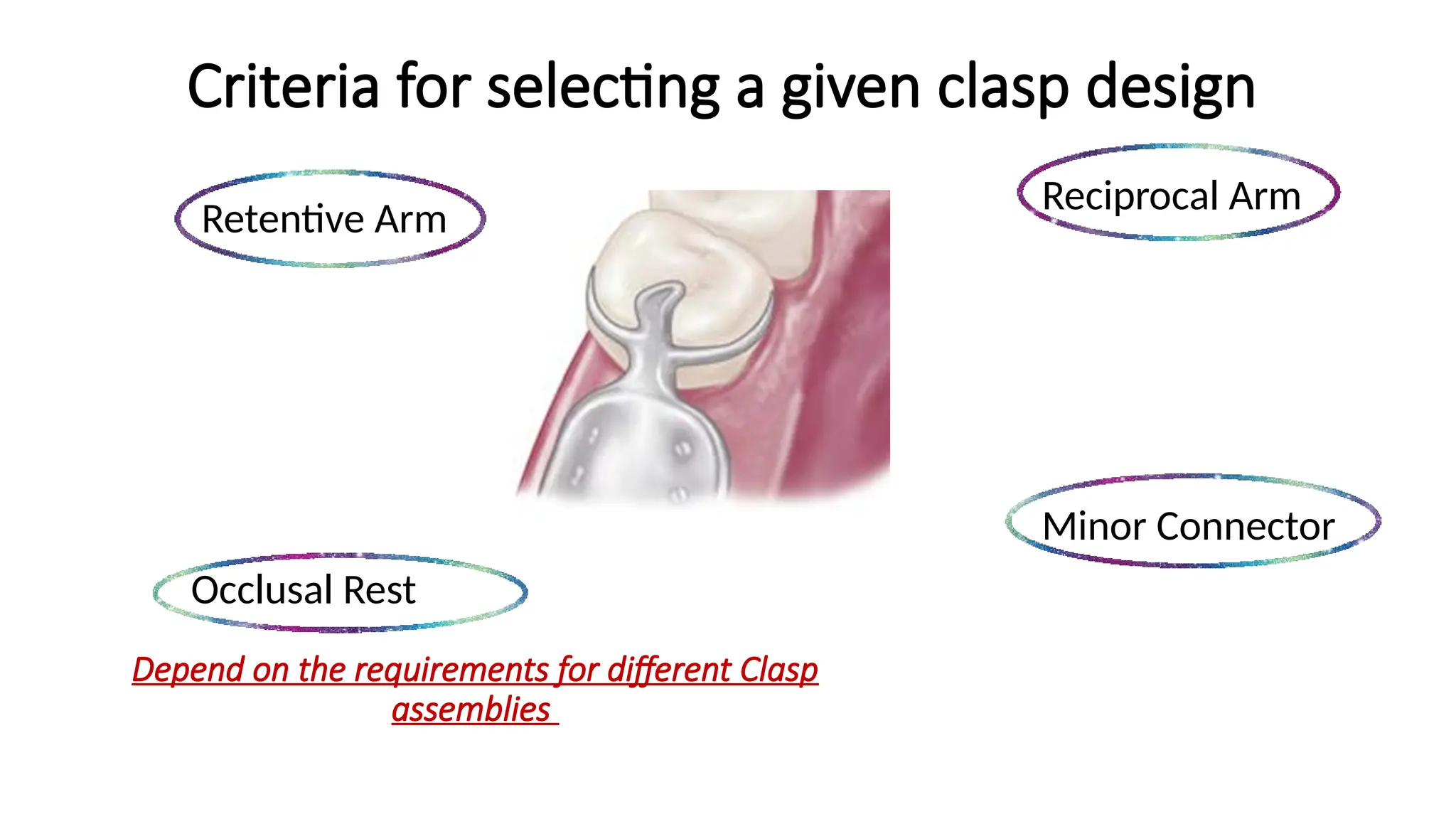
Criteria for selectinga given clasp design
Retentive Arm
Minor Connector
Occlusal Rest
Reciprocal Arm
Depend on the requirements for different Clasp
assemblies
13.
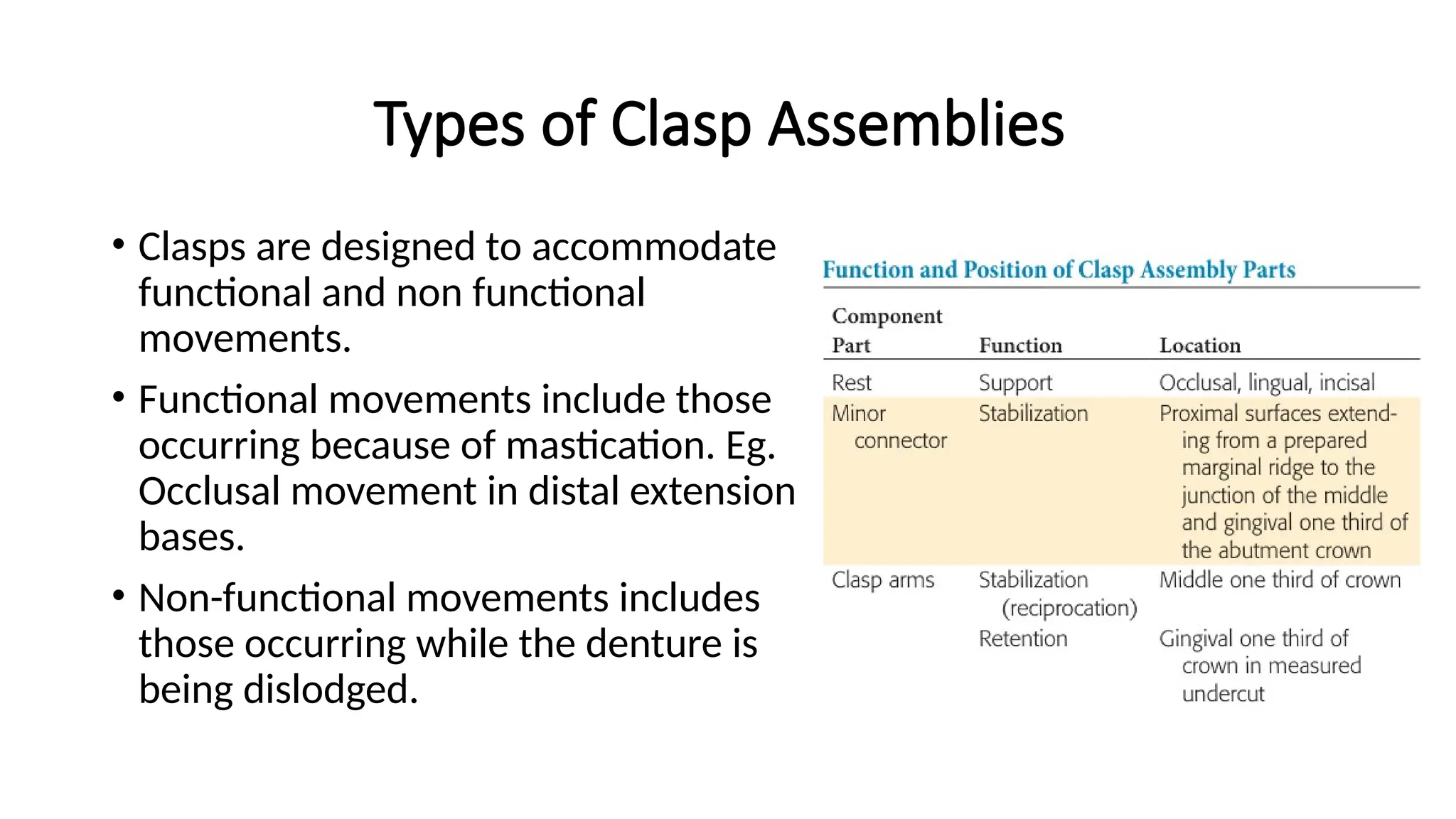
Types of ClaspAssemblies
• Clasps are designed to accommodate
functional and non functional
movements.
• Functional movements include those
occurring because of mastication. Eg.
Occlusal movement in distal extension
bases.
• Non-functional movements includes
those occurring while the denture is
being dislodged.
14.
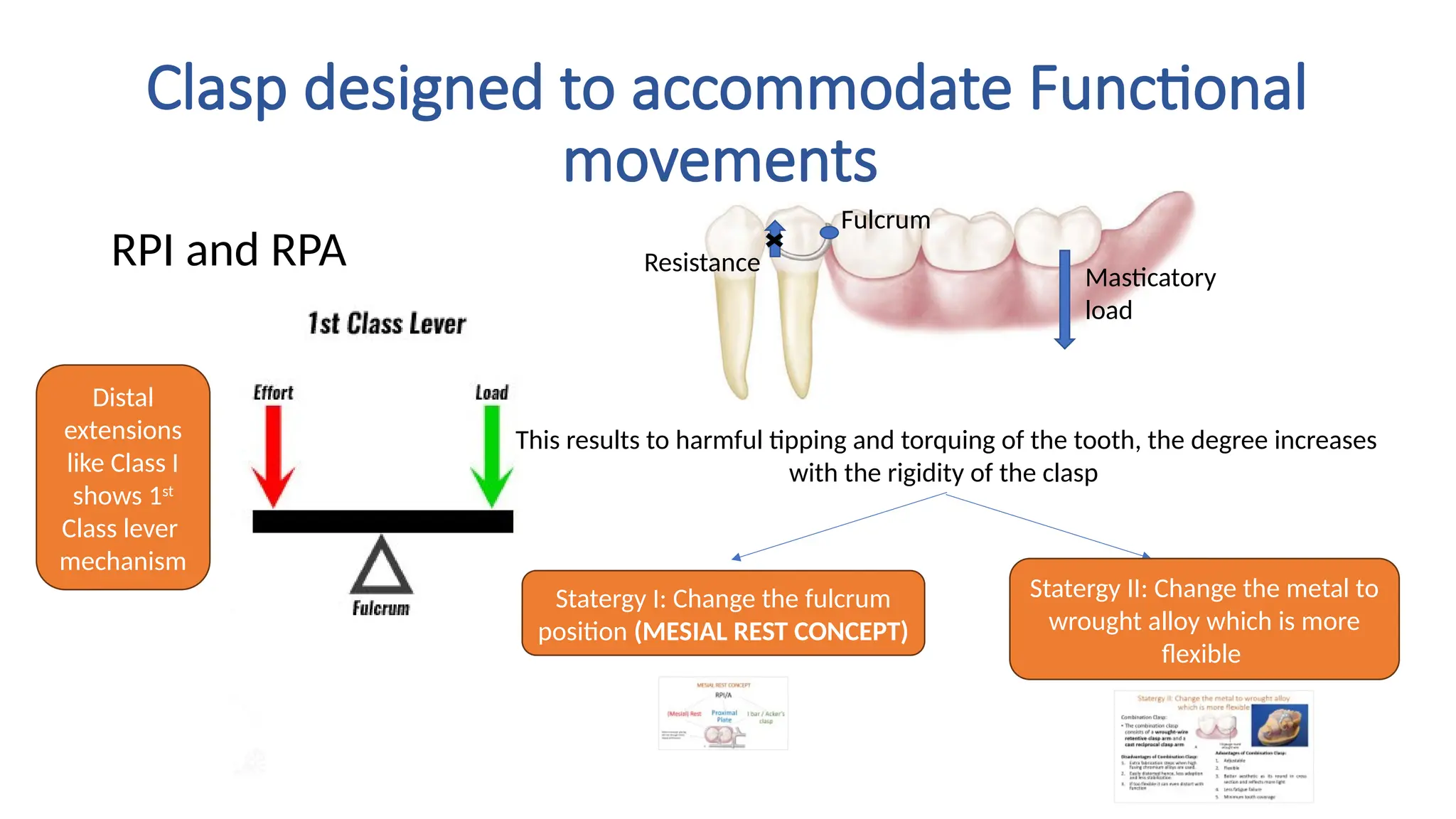
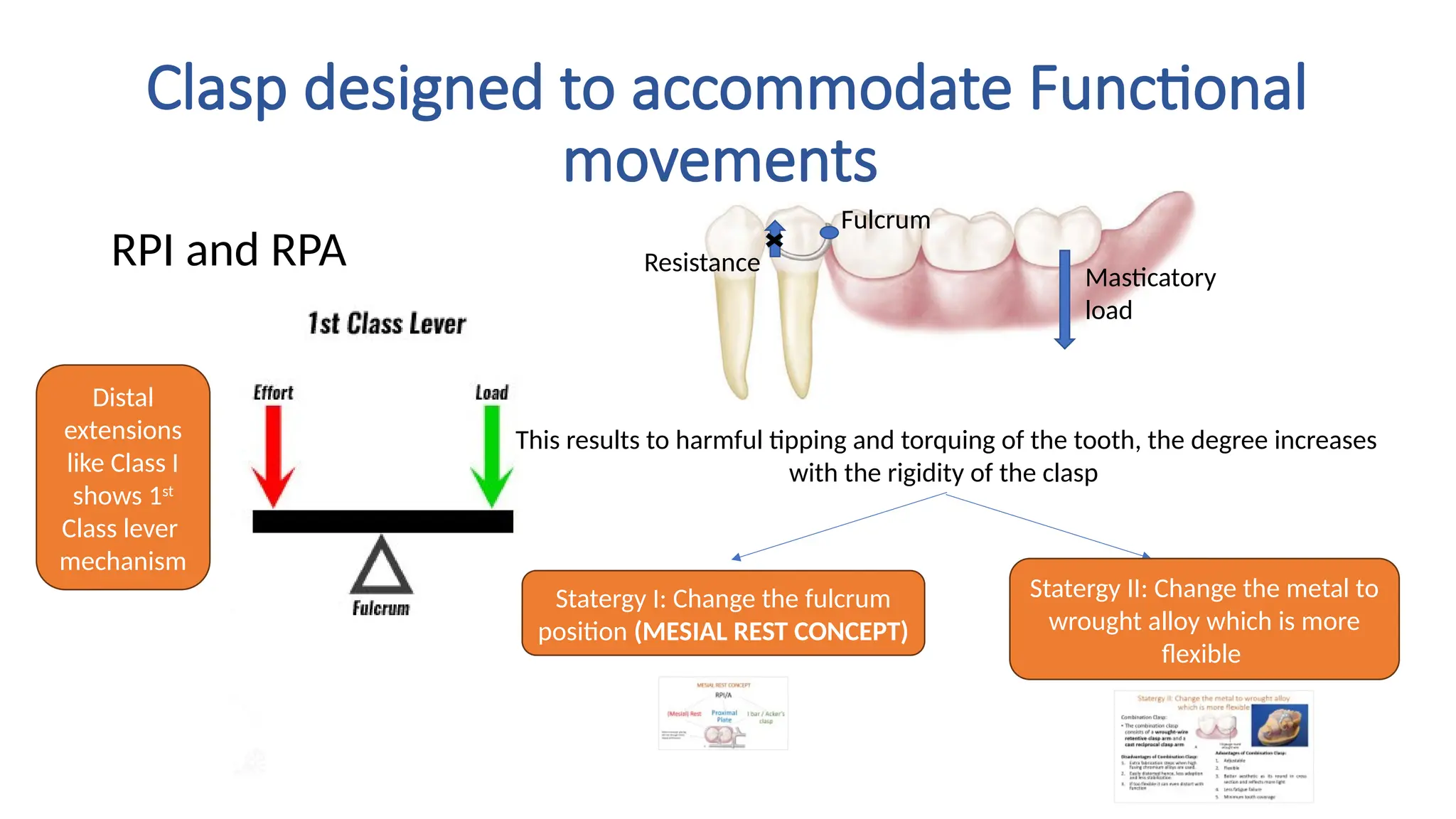
Clasp designed toaccommodate Functional
movements
RPI and RPA Resistance
Fulcrum
Masticatory
load
This results to harmful tipping and torquing of the tooth, the degree increases
with the rigidity of the clasp
Statergy I: Change the fulcrum
position (MESIAL REST CONCEPT)
Statergy II: Change the metal to
wrought alloy which is more
flexible
Distal
extensions
like Class I
shows 1st
Class lever
mechanism
15.
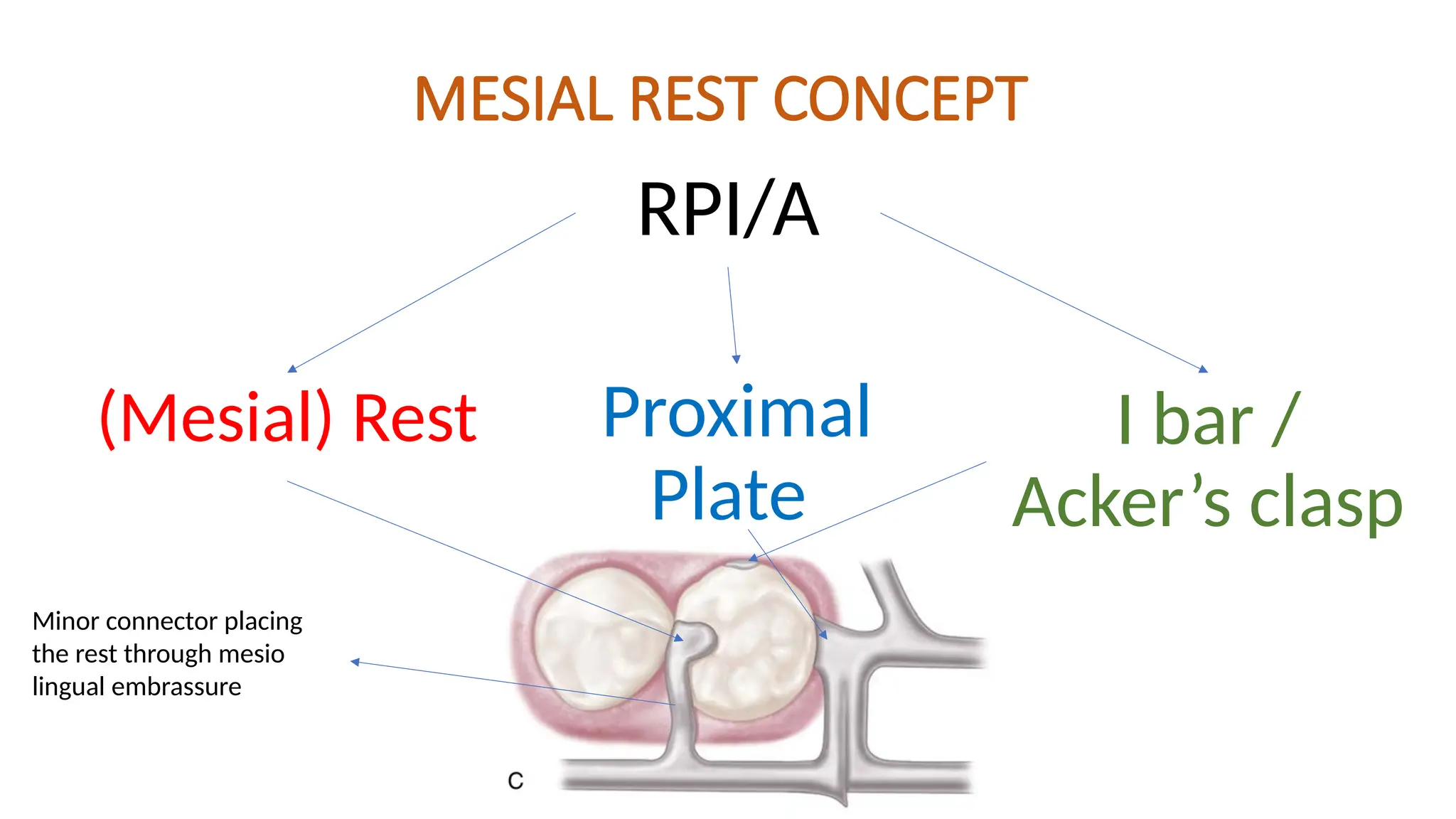
MESIAL REST CONCEPT
RPI/A
(Mesial)Rest Proximal
Plate
I bar /
Acker’s clasp
Minor connector placing
the rest through mesio
lingual embrassure
16.
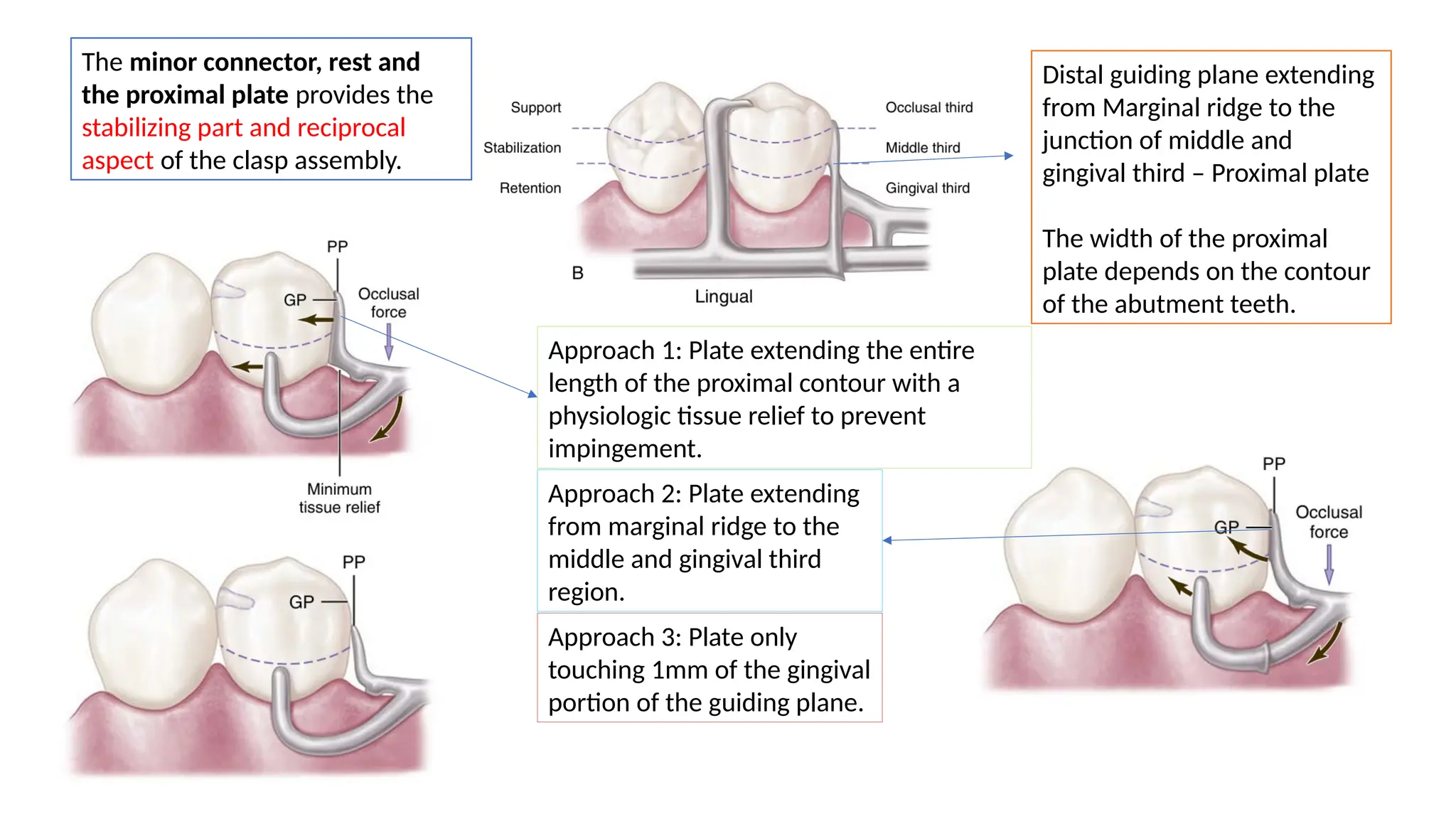
Distal guiding planeextending
from Marginal ridge to the
junction of middle and
gingival third – Proximal plate
The width of the proximal
plate depends on the contour
of the abutment teeth.
The minor connector, rest and
the proximal plate provides the
stabilizing part and reciprocal
aspect of the clasp assembly.
Approach 1: Plate extending the entire
length of the proximal contour with a
physiologic tissue relief to prevent
impingement.
Approach 2: Plate extending
from marginal ridge to the
middle and gingival third
region.
Approach 3: Plate only
touching 1mm of the gingival
portion of the guiding plane.
17.
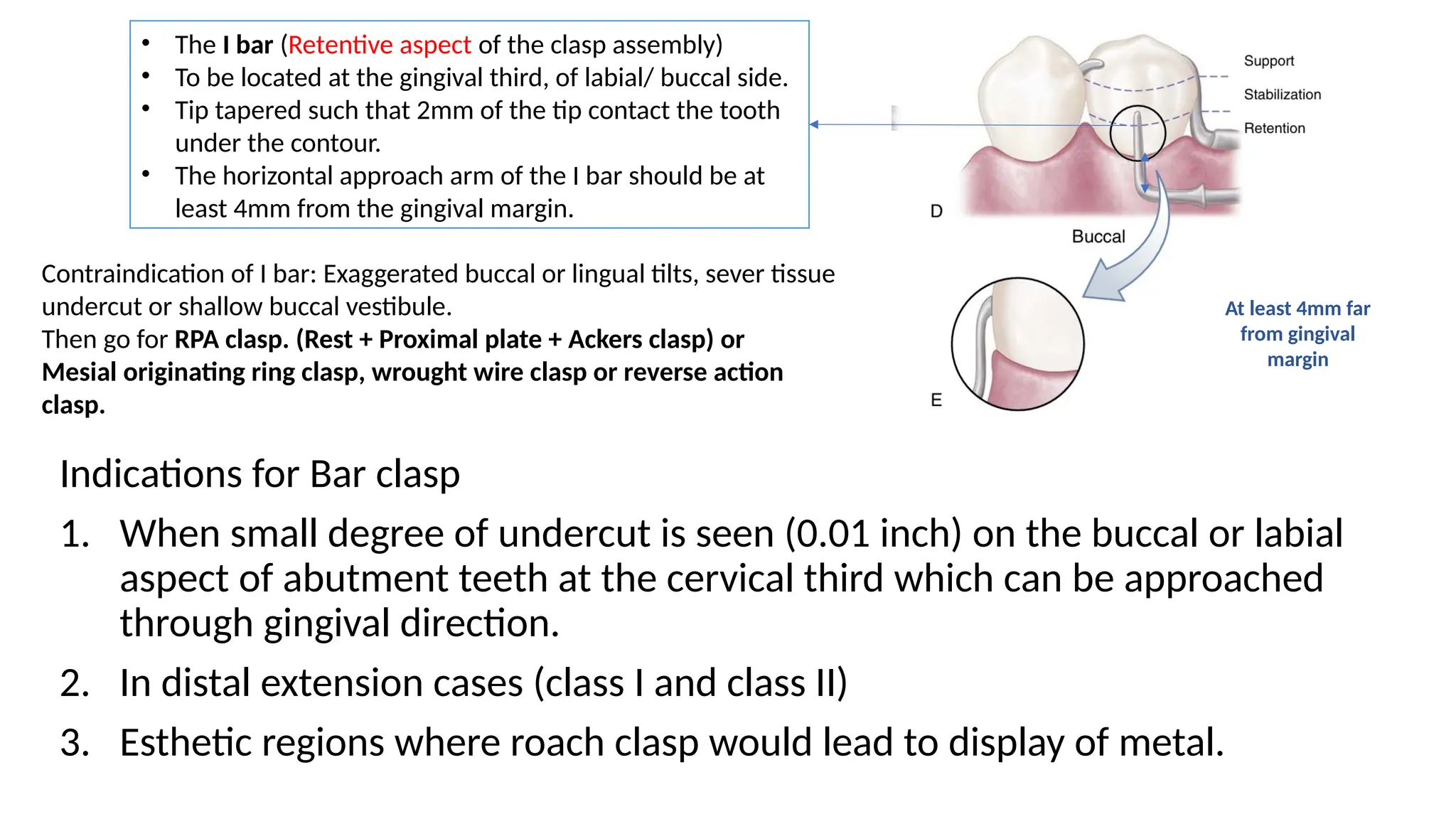
• The Ibar (Retentive aspect of the clasp assembly)
• To be located at the gingival third, of labial/ buccal side.
• Tip tapered such that 2mm of the tip contact the tooth
under the contour.
• The horizontal approach arm of the I bar should be at
least 4mm from the gingival margin.
At least 4mm far
from gingival
margin
Contraindication of I bar: Exaggerated buccal or lingual tilts, sever tissue
undercut or shallow buccal vestibule.
Then go for RPA clasp. (Rest + Proximal plate + Ackers clasp) or
Mesial originating ring clasp, wrought wire clasp or reverse action
clasp.
Indications for Bar clasp
1. When small degree of undercut is seen (0.01 inch) on the buccal or labial
aspect of abutment teeth at the cervical third which can be approached
through gingival direction.
2. In distal extension cases (class I and class II)
3. Esthetic regions where roach clasp would lead to display of metal.
18.
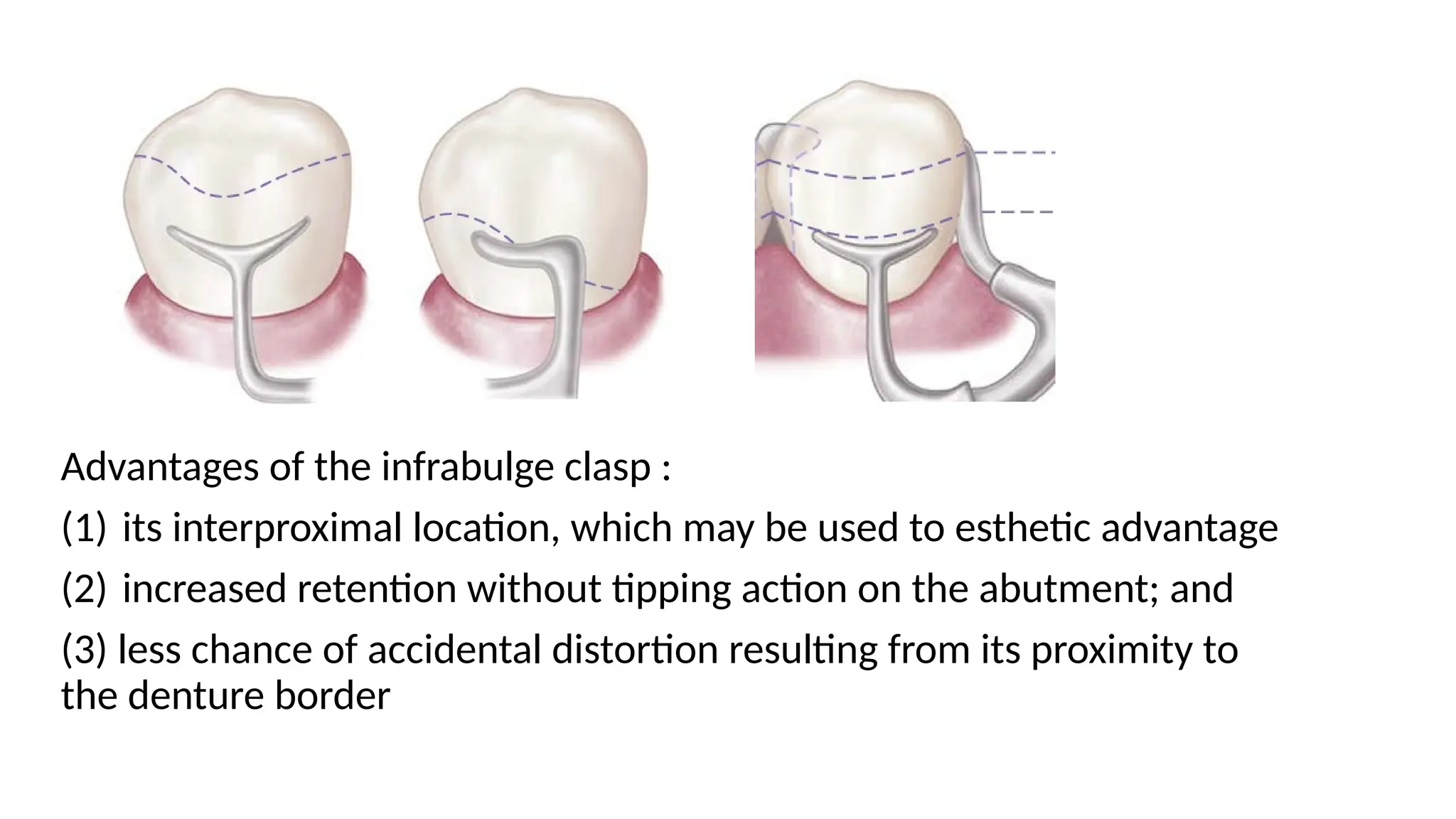
Advantages of theinfrabulge clasp :
(1) its interproximal location, which may be used to esthetic advantage
(2) increased retention without tipping action on the abutment; and
(3) less chance of accidental distortion resulting from its proximity to
the denture border
19.
Clasp designed toaccommodate Functional
movements
RPI and RPA Resistance
Fulcrum
Masticatory
load
This results to harmful tipping and torquing of the tooth, the degree increases
with the rigidity of the clasp
Statergy I: Change the fulcrum
position (MESIAL REST CONCEPT)
Statergy II: Change the metal to
wrought alloy which is more
flexible
Distal
extensions
like Class I
shows 1st
Class lever
mechanism
20.
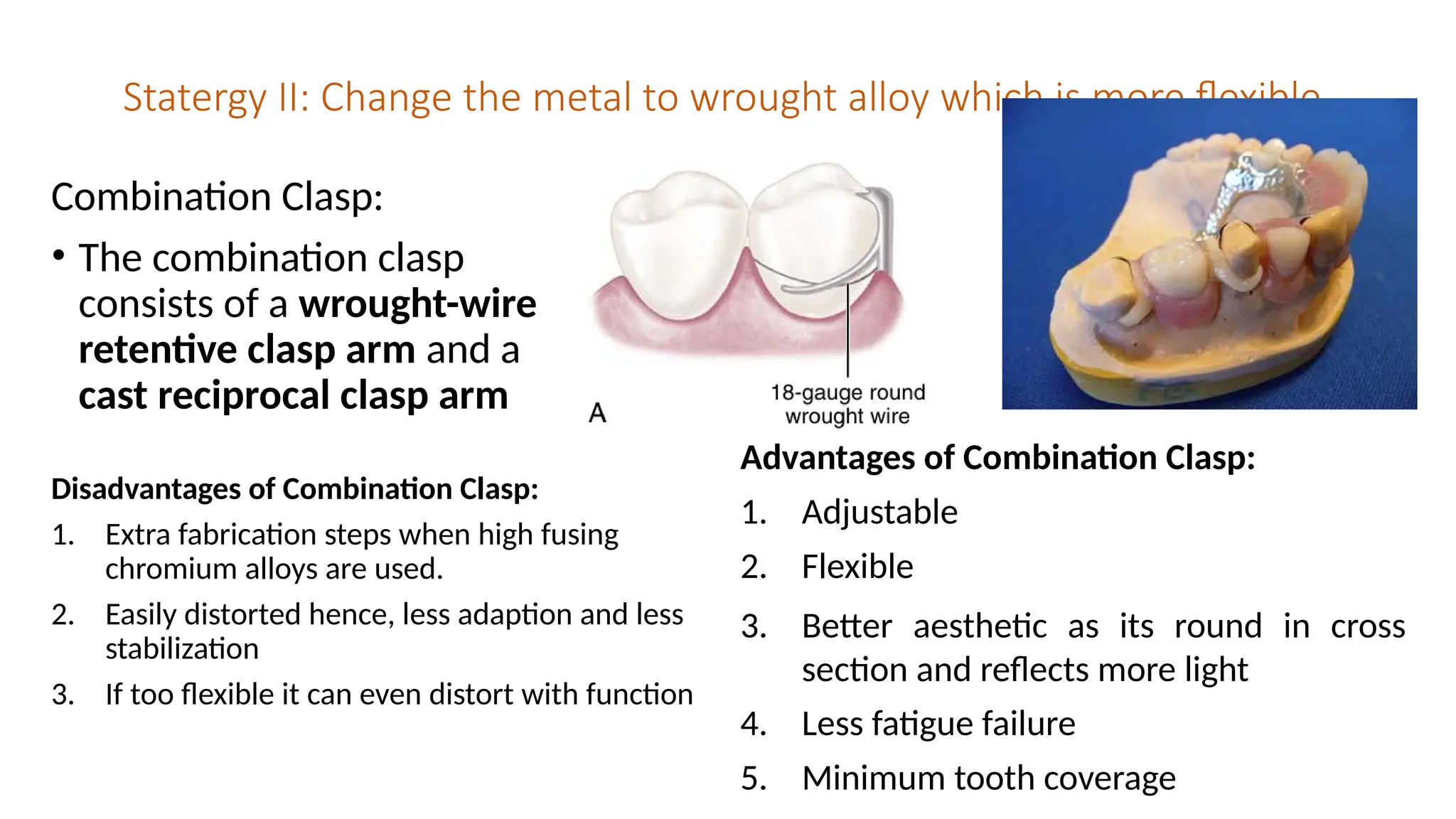
Statergy II: Changethe metal to wrought alloy which is more flexible
Combination Clasp:
• The combination clasp
consists of a wrought-wire
retentive clasp arm and a
cast reciprocal clasp arm
Disadvantages of Combination Clasp:
1. Extra fabrication steps when high fusing
chromium alloys are used.
2. Easily distorted hence, less adaption and less
stabilization
3. If too flexible it can even distort with function
Advantages of Combination Clasp:
1. Adjustable
2. Flexible
3. Better aesthetic as its round in cross
section and reflects more light
4. Less fatigue failure
5. Minimum tooth coverage
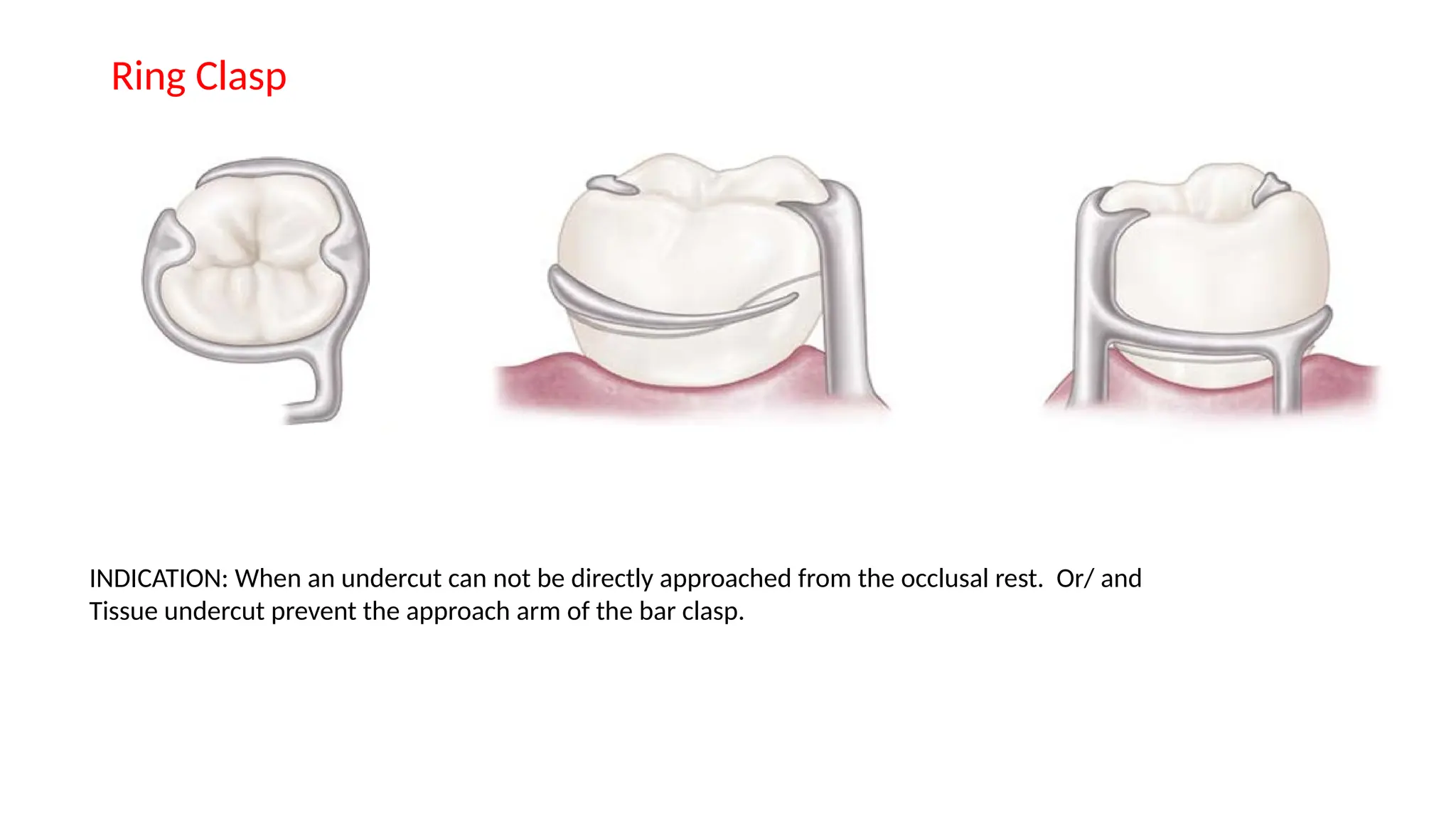
Ring Clasp
INDICATION: Whenan undercut can not be directly approached from the occlusal rest. Or/ and
Tissue undercut prevent the approach arm of the bar clasp.
24.
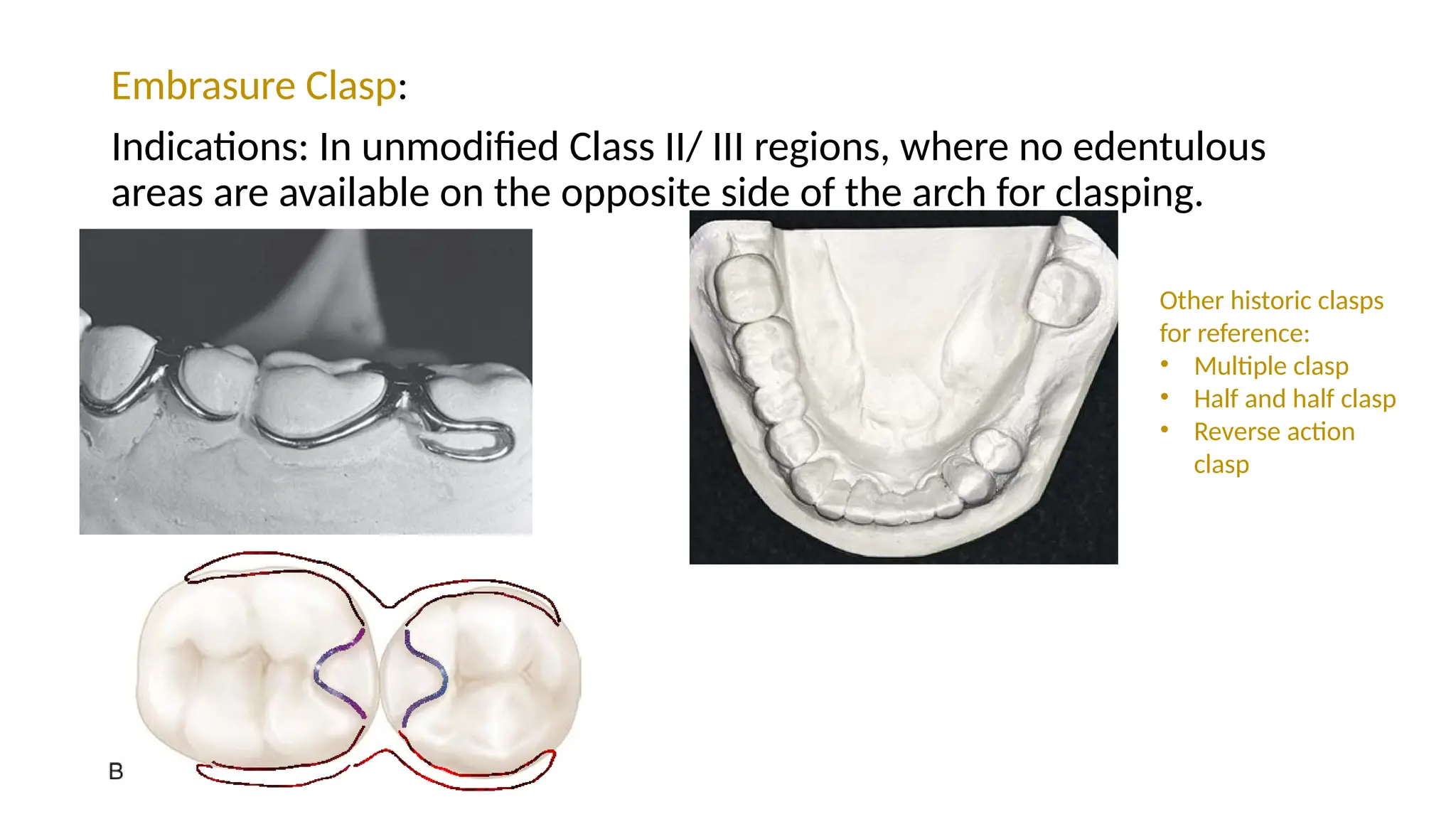
Embrasure Clasp:
Indications: Inunmodified Class II/ III regions, where no edentulous
areas are available on the opposite side of the arch for clasping.
Other historic clasps
for reference:
• Multiple clasp
• Half and half clasp
• Reverse action
clasp
25.
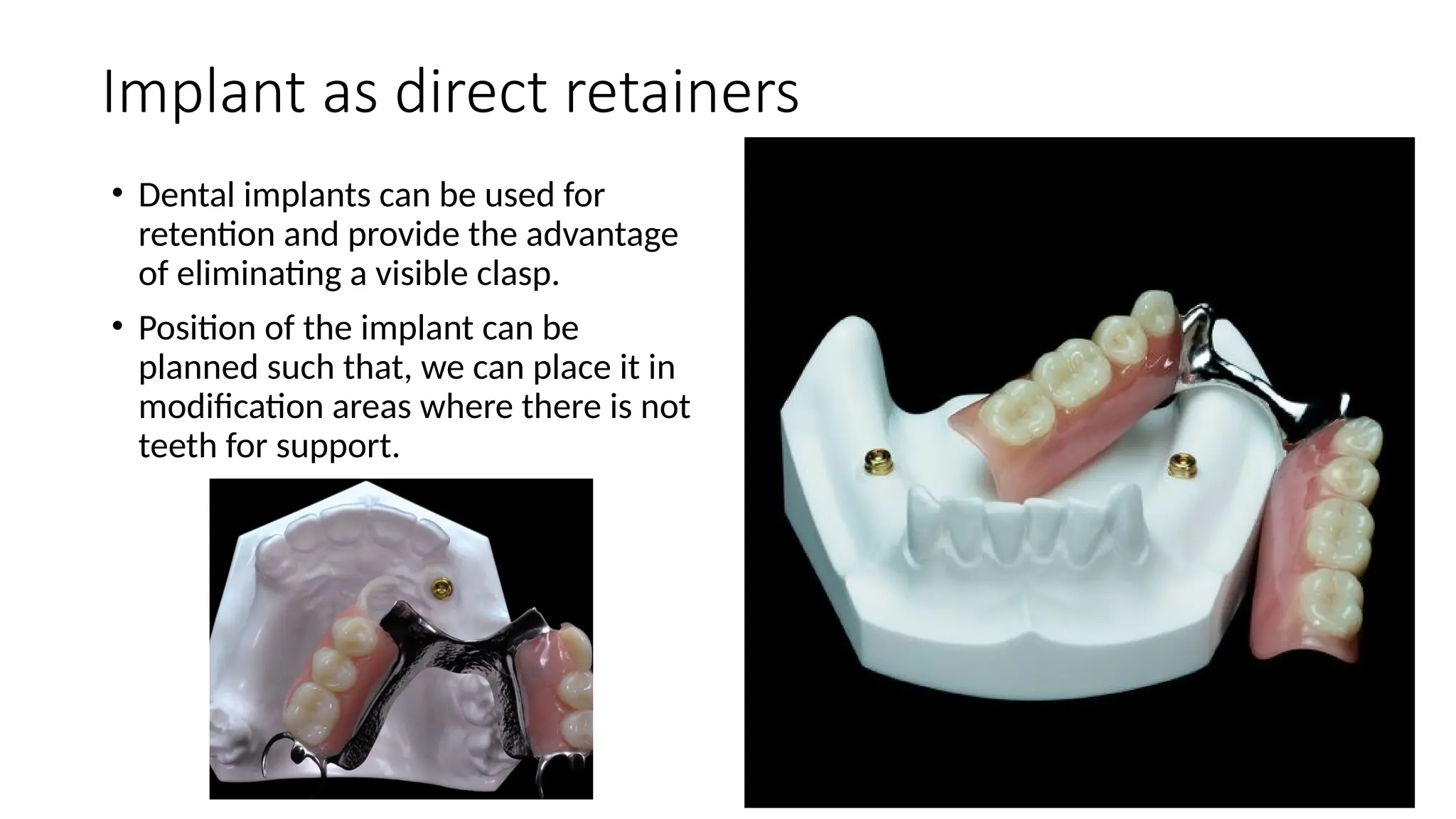
Implant as directretainers
• Dental implants can be used for
retention and provide the advantage
of eliminating a visible clasp.
• Position of the implant can be
planned such that, we can place it in
modification areas where there is not
teeth for support.
26.
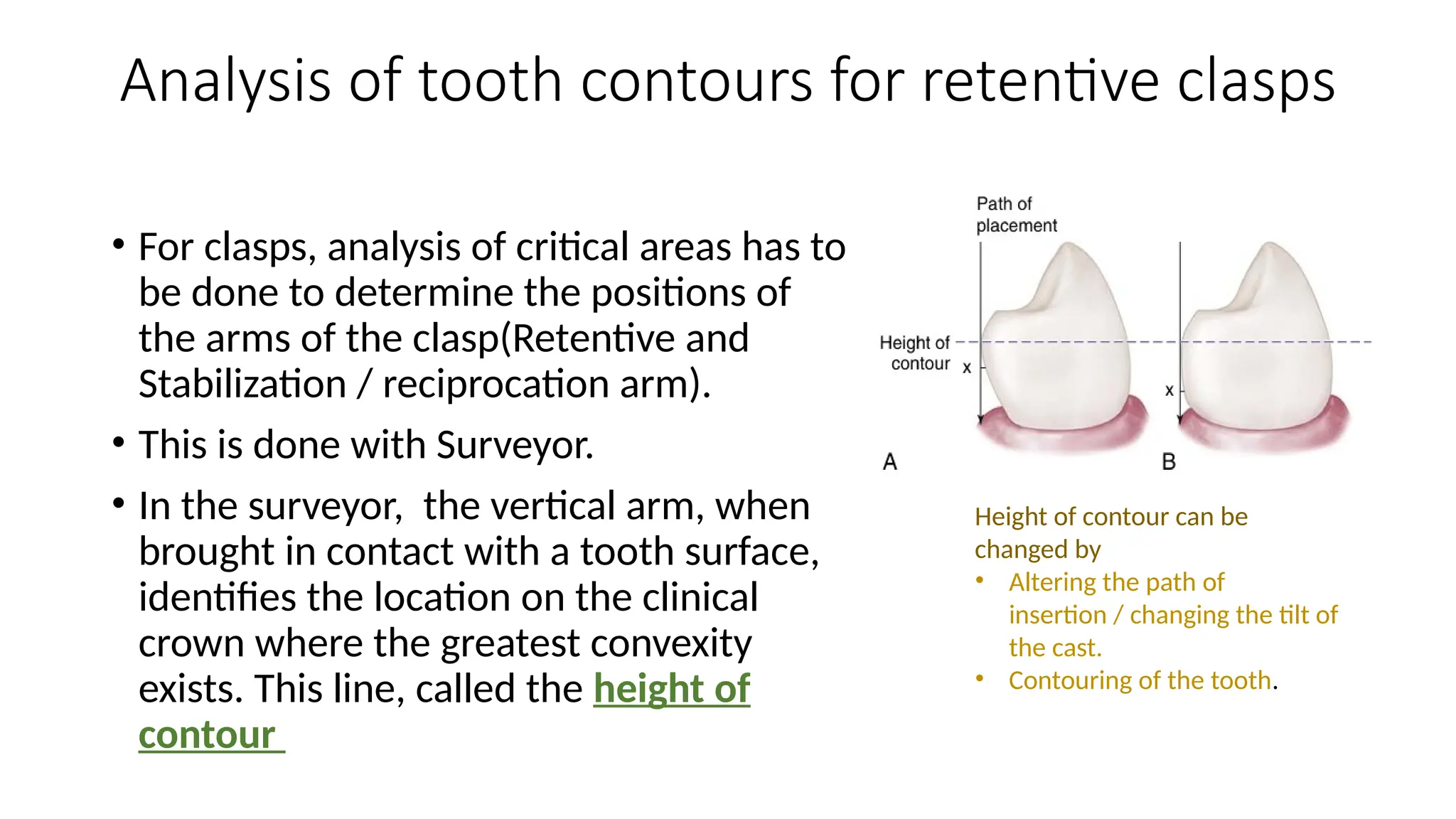
Analysis of toothcontours for retentive clasps
• For clasps, analysis of critical areas has to
be done to determine the positions of
the arms of the clasp(Retentive and
Stabilization / reciprocation arm).
• This is done with Surveyor.
• In the surveyor, the vertical arm, when
brought in contact with a tooth surface,
identifies the location on the clinical
crown where the greatest convexity
exists. This line, called the height of
contour
Height of contour can be
changed by
• Altering the path of
insertion / changing the tilt of
the cast.
• Contouring of the tooth.
27.
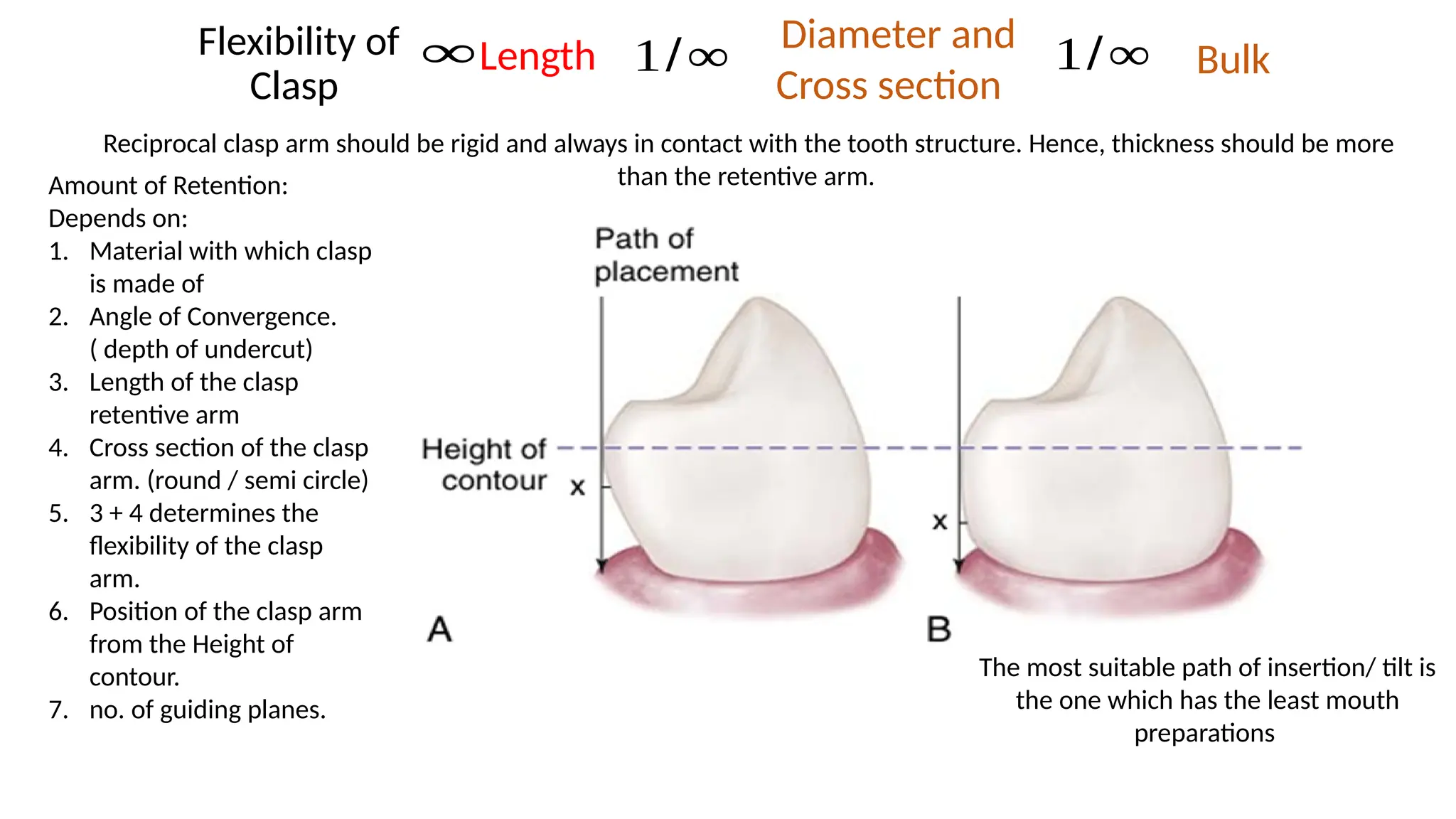
Amount of Retention:
Dependson:
1. Material with which clasp
is made of
2. Angle of Convergence.
( depth of undercut)
3. Length of the clasp
retentive arm
4. Cross section of the clasp
arm. (round / semi circle)
5. 3 + 4 determines the
flexibility of the clasp
arm.
6. Position of the clasp arm
from the Height of
contour.
7. no. of guiding planes.
The most suitable path of insertion/ tilt is
the one which has the least mouth
preparations
Flexibility of
Clasp
1/∞
Length
∞ Diameter and
Cross section
1/∞ Bulk
Reciprocal clasp arm should be rigid and always in contact with the tooth structure. Hence, thickness should be more
than the retentive arm.
28.
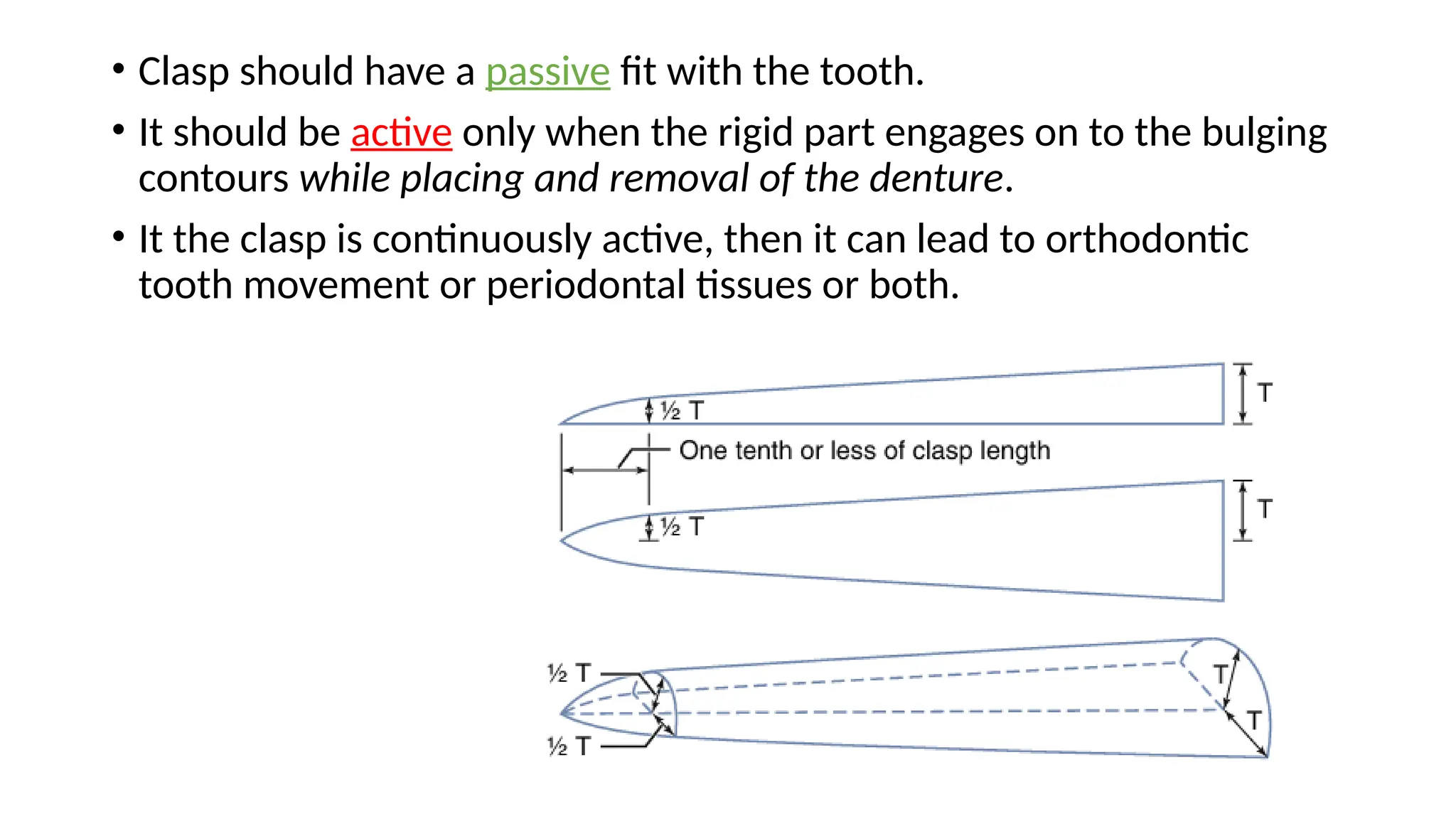
• Clasp shouldhave a passive fit with the tooth.
• It should be active only when the rigid part engages on to the bulging
contours while placing and removal of the denture.
• It the clasp is continuously active, then it can lead to orthodontic
tooth movement or periodontal tissues or both.
29.
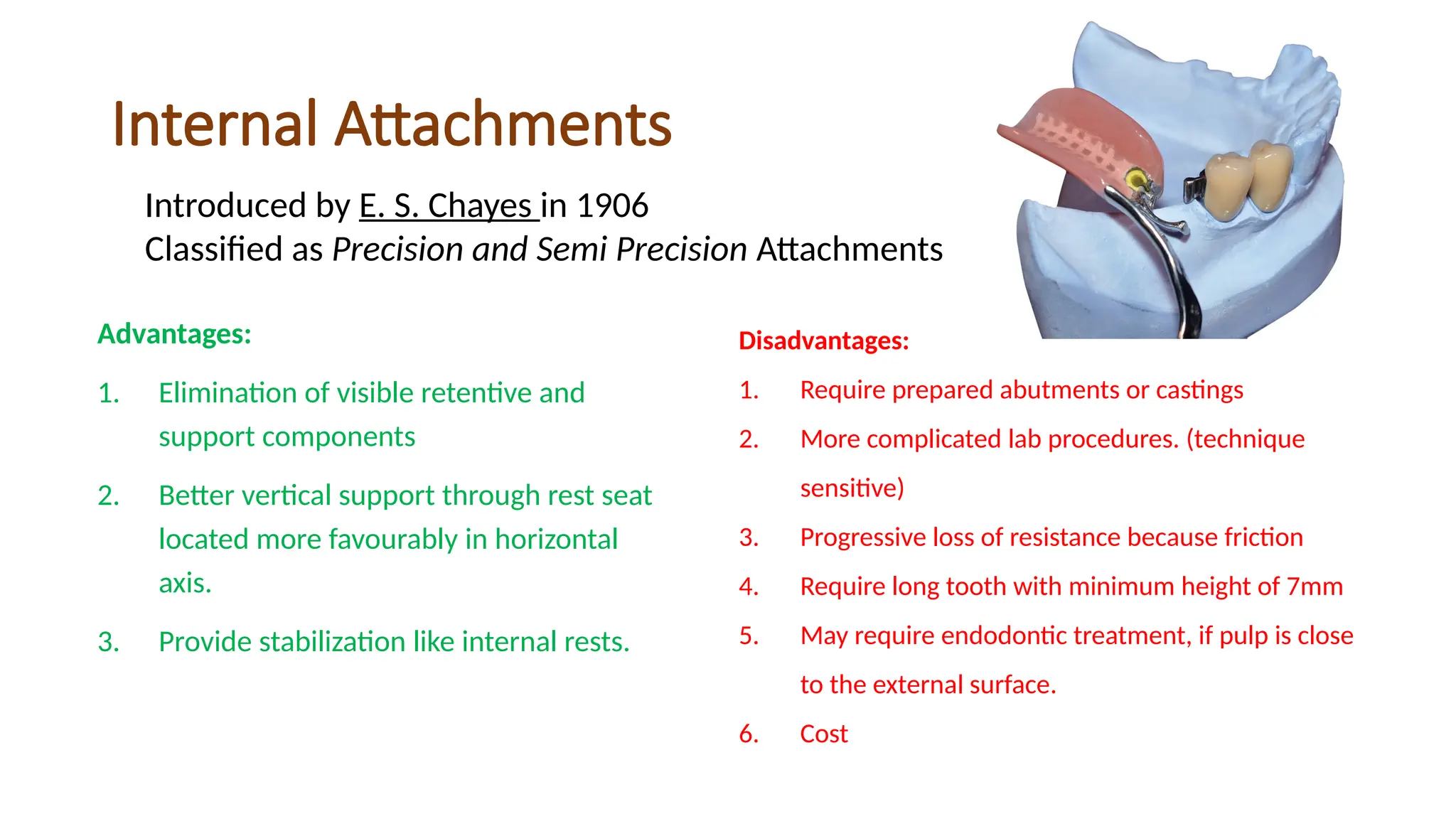
Internal Attachments
Advantages:
1. Eliminationof visible retentive and
support components
2. Better vertical support through rest seat
located more favourably in horizontal
axis.
3. Provide stabilization like internal rests.
Introduced by E. S. Chayes in 1906
Classified as Precision and Semi Precision Attachments
Disadvantages:
1. Require prepared abutments or castings
2. More complicated lab procedures. (technique
sensitive)
3. Progressive loss of resistance because friction
4. Require long tooth with minimum height of 7mm
5. May require endodontic treatment, if pulp is close
to the external surface.
6. Cost
30.
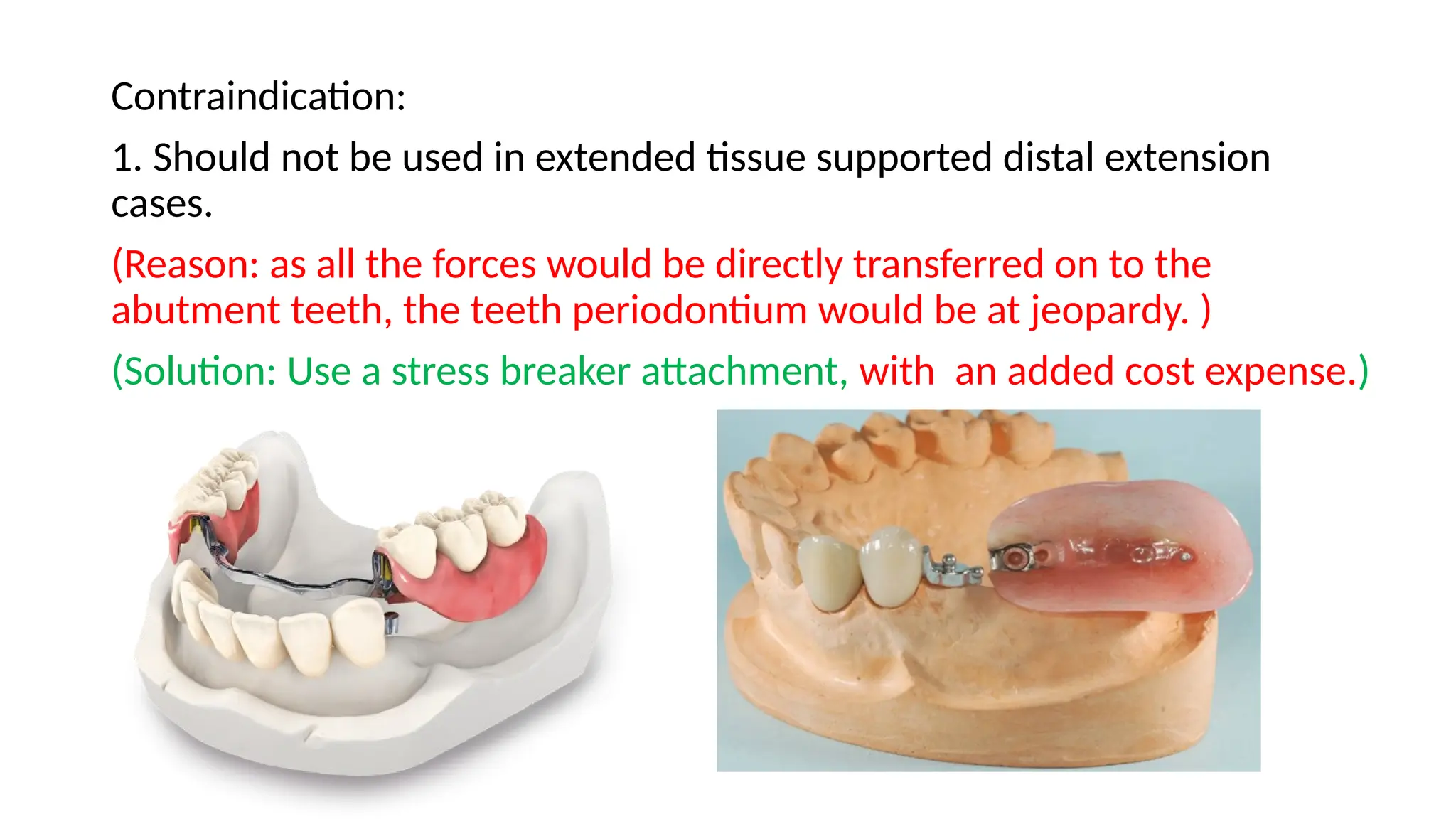
Contraindication:
1. Should notbe used in extended tissue supported distal extension
cases.
(Reason: as all the forces would be directly transferred on to the
abutment teeth, the teeth periodontium would be at jeopardy. )
(Solution: Use a stress breaker attachment, with an added cost expense.)
31.
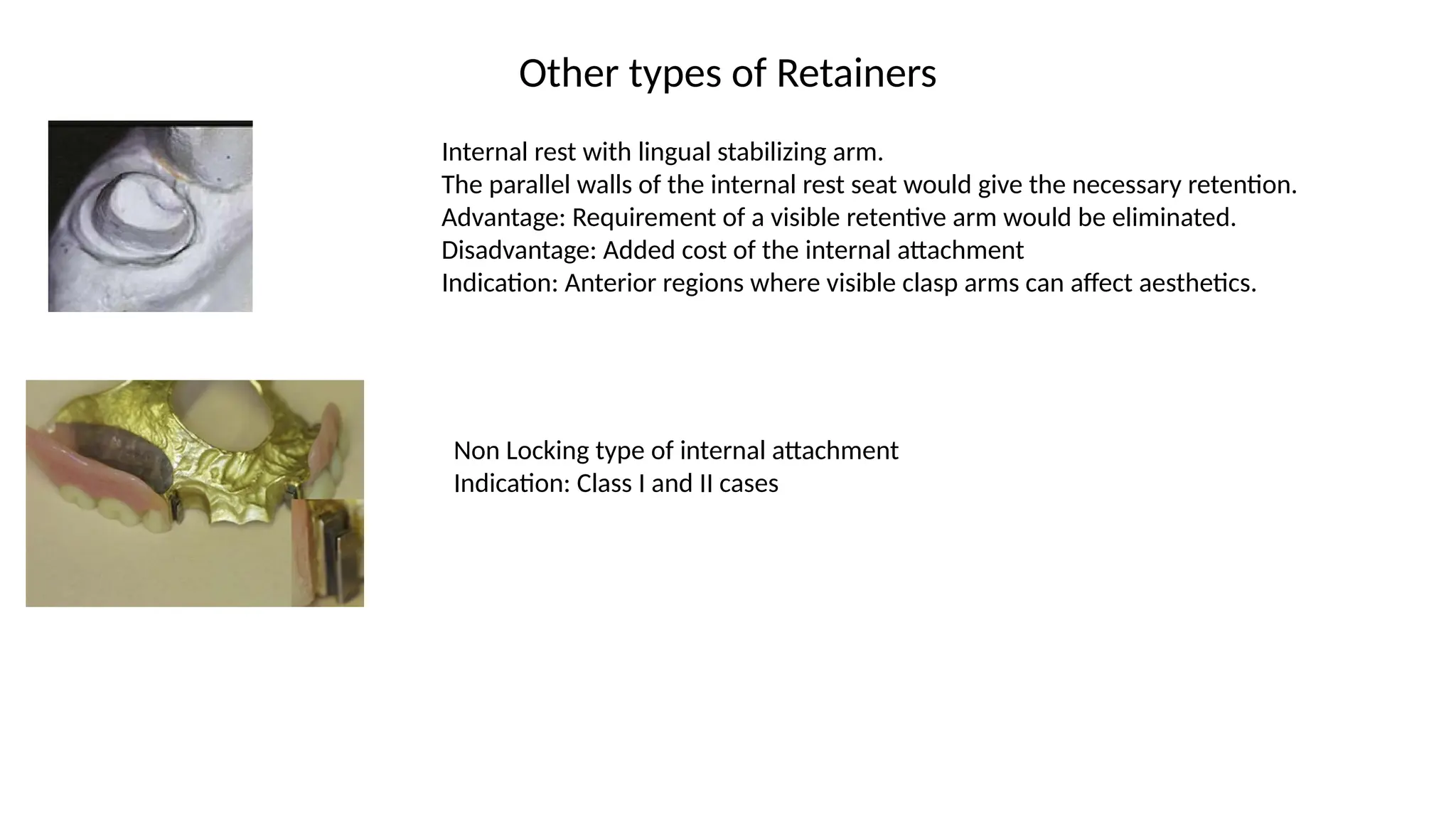
Other types ofRetainers
Internal rest with lingual stabilizing arm.
The parallel walls of the internal rest seat would give the necessary retention.
Advantage: Requirement of a visible retentive arm would be eliminated.
Disadvantage: Added cost of the internal attachment
Indication: Anterior regions where visible clasp arms can affect aesthetics.
Non Locking type of internal attachment
Indication: Class I and II cases
32.
References
1. Mc CrackenRemovable Partial Prosthodontics Edition 13.
2. Picture Source: Google Search Engine.
32