Downloaded 26 times


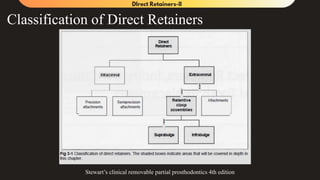
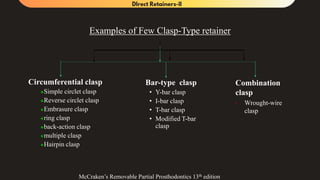




































The document outlines various types of retainer clasps used in removable partial dentures, including suprabulge and infrabulge clasps, their design rules, and clinical applications across different cases such as Kennedy's classes. It emphasizes design philosophies, specific clasp types, their advantages, limitations, and the scientific studies supporting these practices in the context of prosthodontics. Additionally, it discusses the importance of guiding planes, occlusal rests, and the impact of clasp design on abutment tooth movement.








































![RPI System [Autosaved].ppt.;lkjhughgfxdcvbjkl;](https://cdn.slidesharecdn.com/ss_thumbnails/rpisystemautosaved-241021162716-5b5a84ab-thumbnail.jpg?width=640&height=640&fit=bounds)



































