Downloaded 893 times
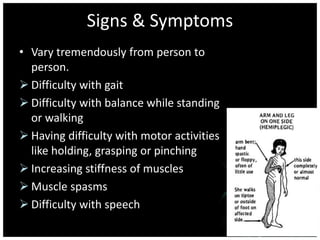



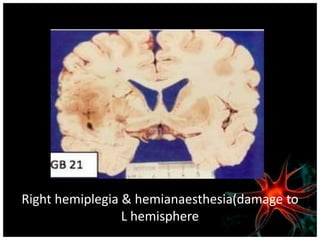




Hemiplegia is the total paralysis of one side of the body that can be caused by stroke, head trauma, brain tumors, or other neurological conditions. It is characterized by an inability to voluntarily move the arm, leg, and trunk on the same side of the body. Symptoms vary but can include difficulties with walking, balance, grasping objects, muscle stiffness, spasms, and speech or swallowing. Treatment involves rehabilitation to help regain motor function through exercises and may include pharmacological interventions or surgery depending on the underlying cause.