Downloaded 3,076 times










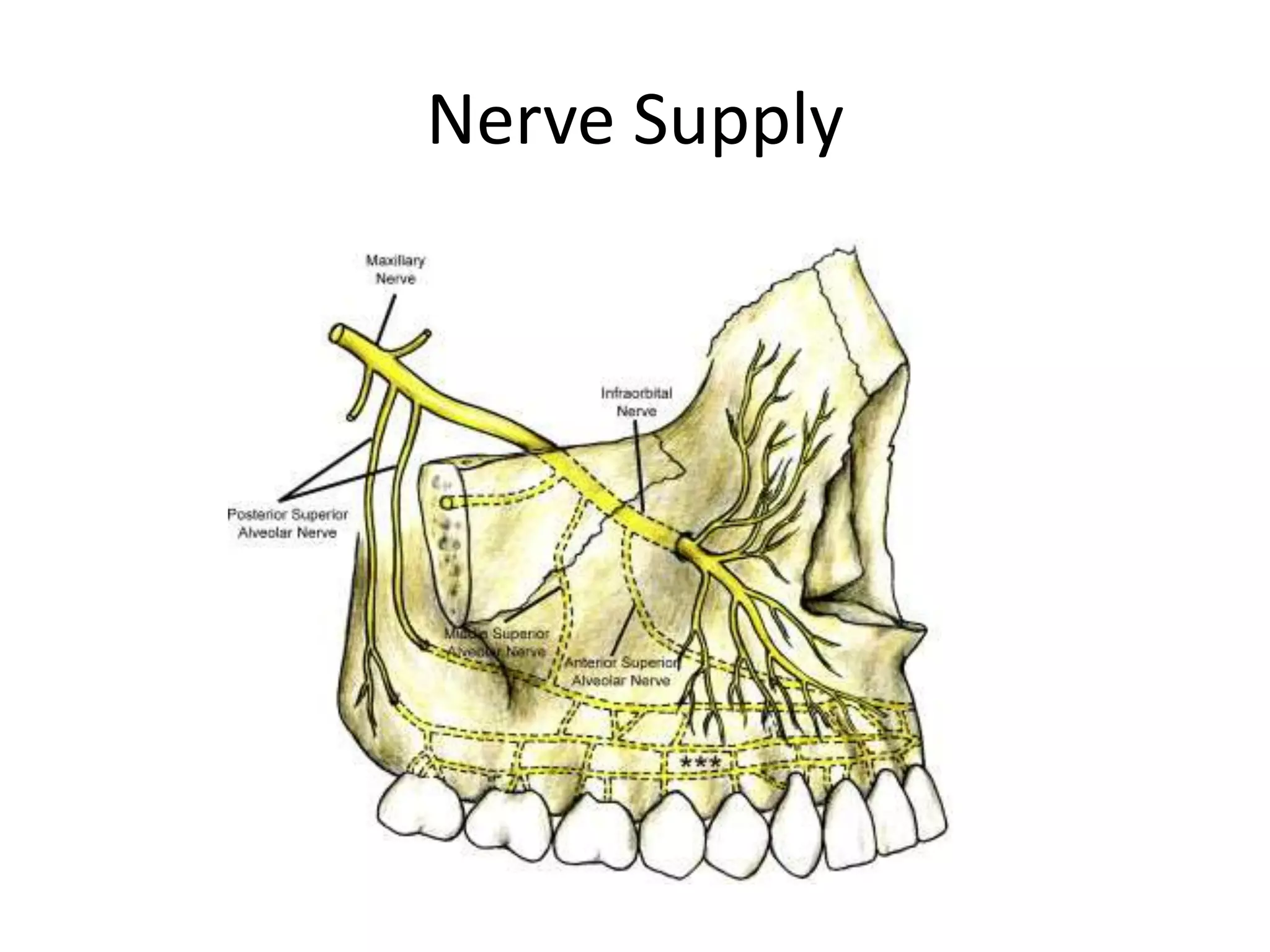


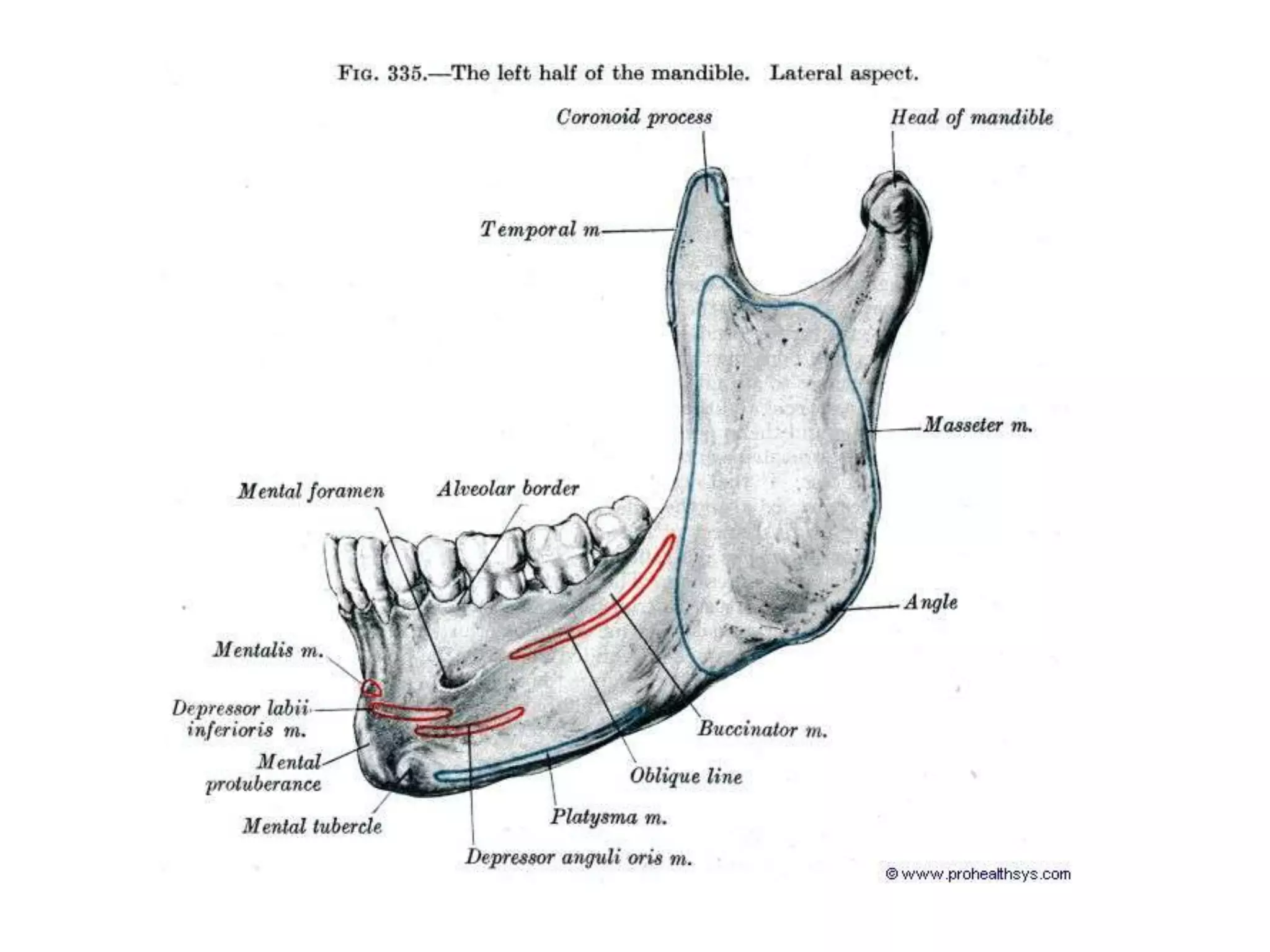
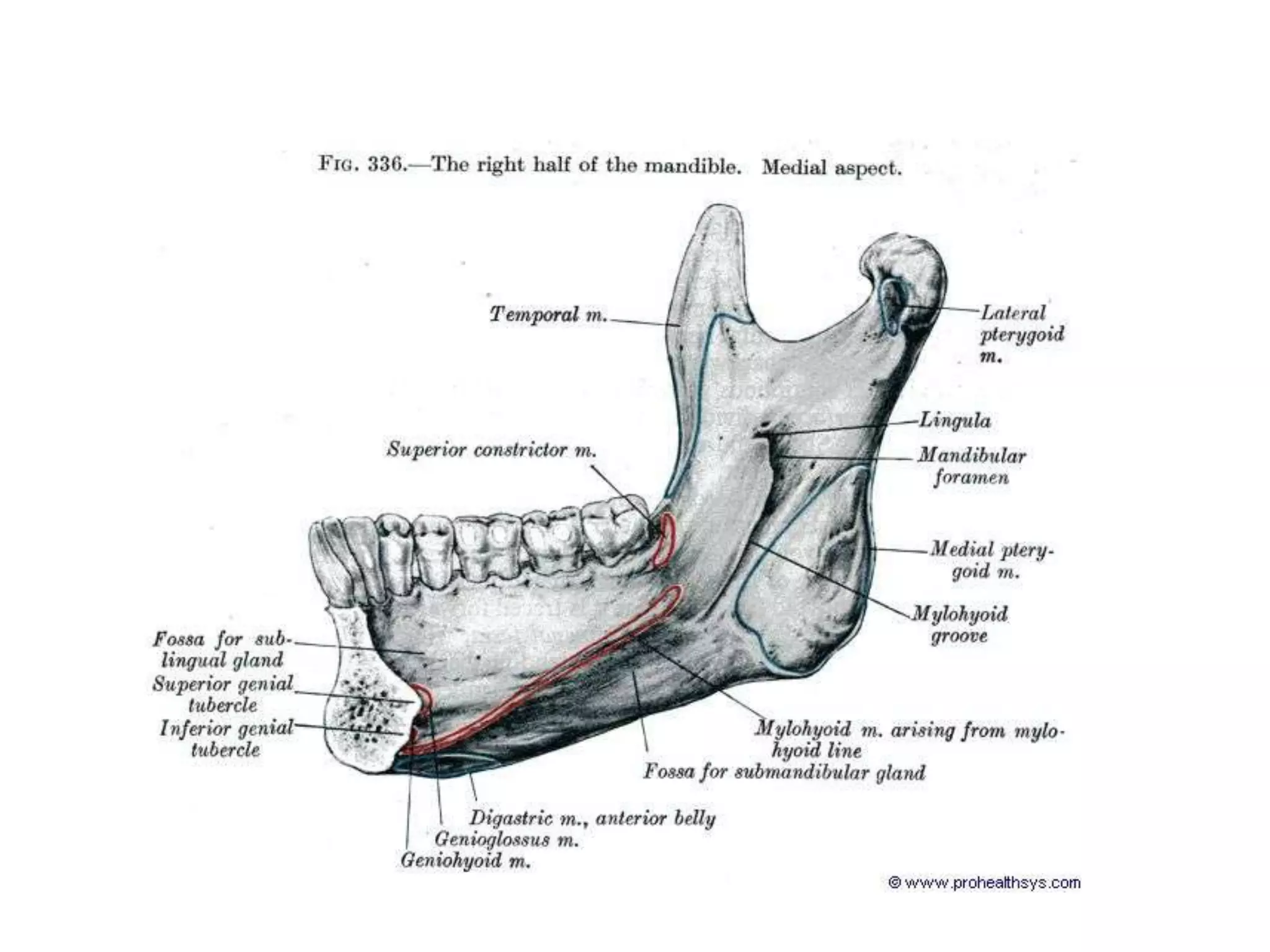






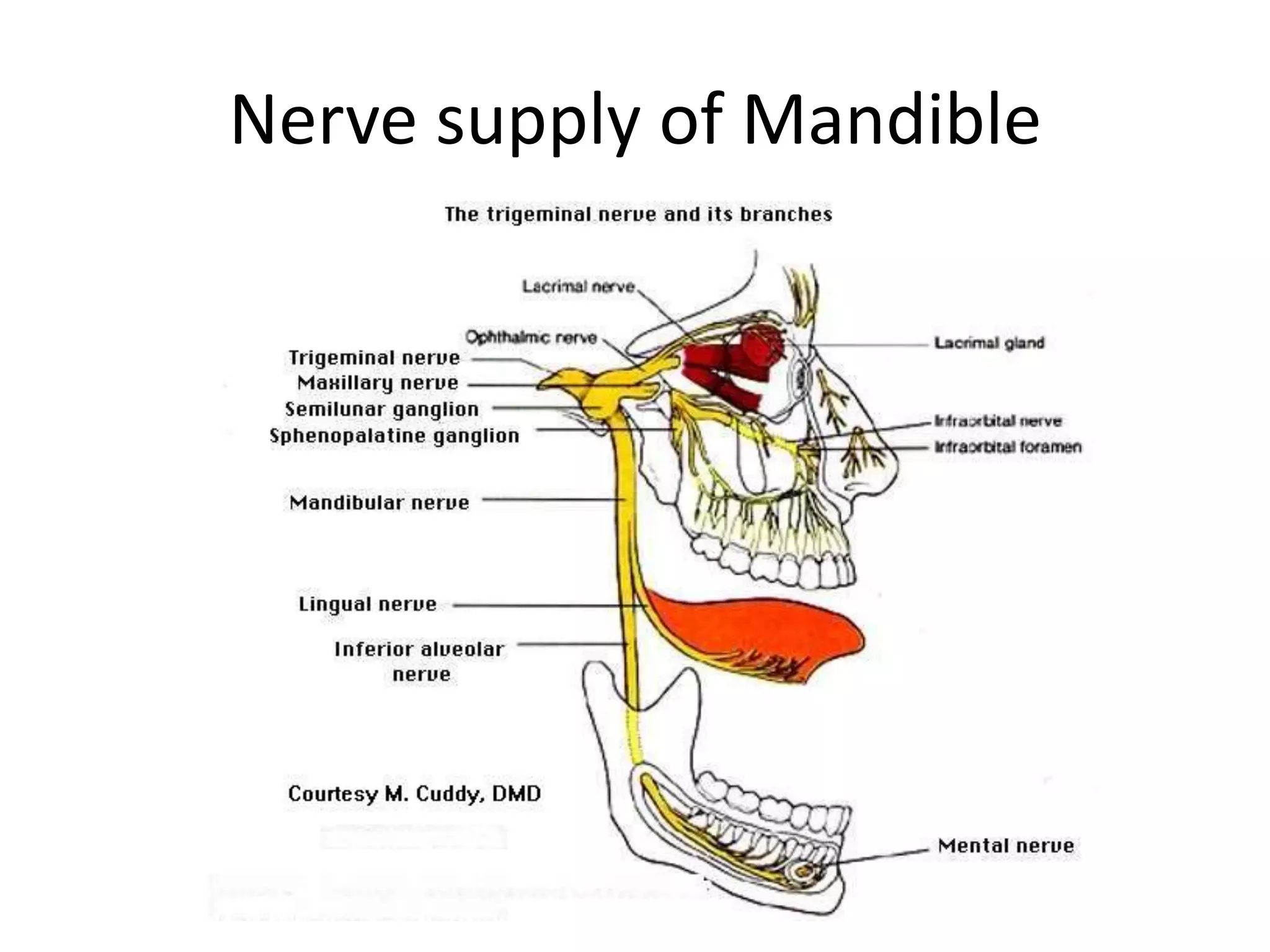
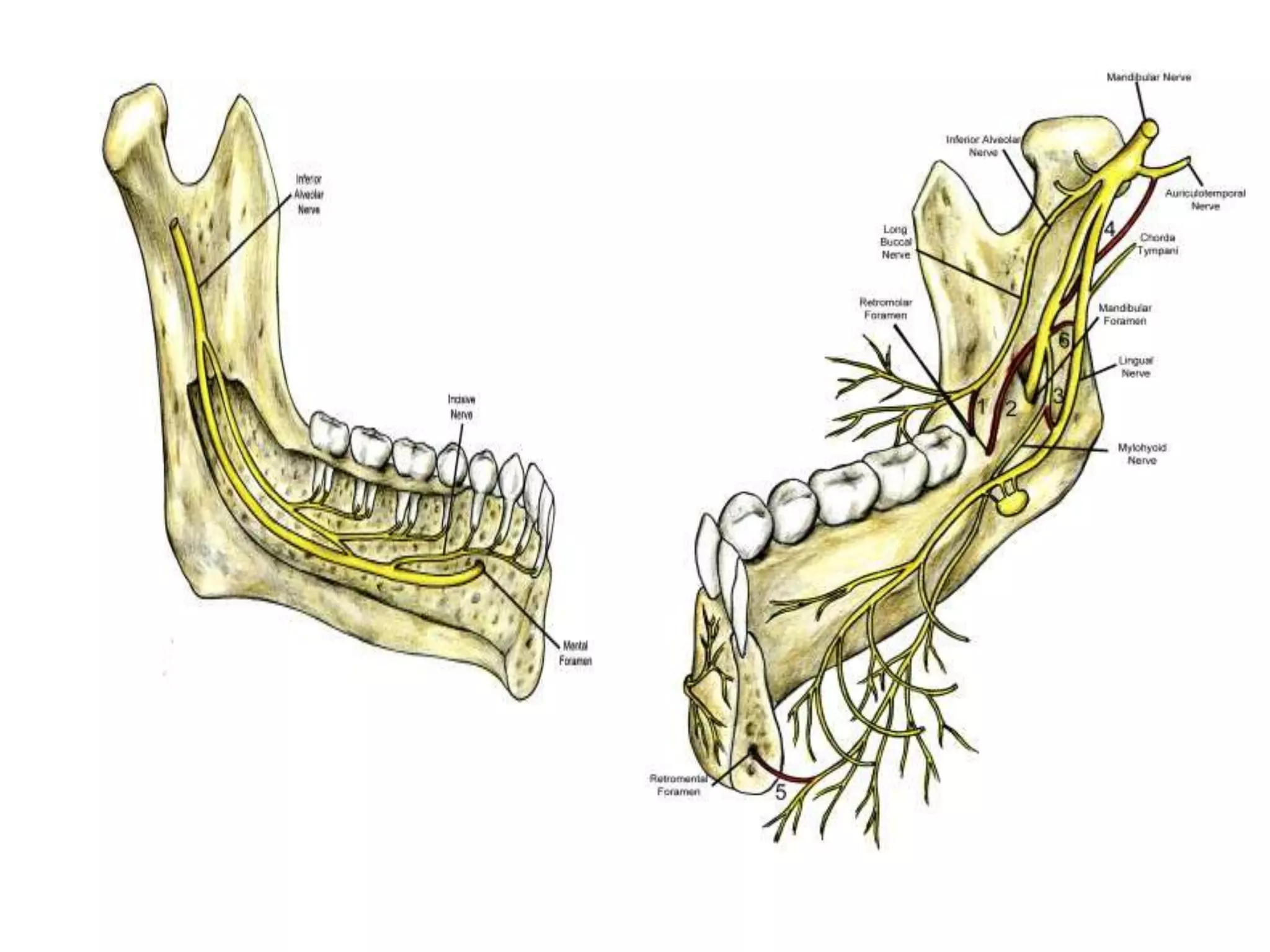
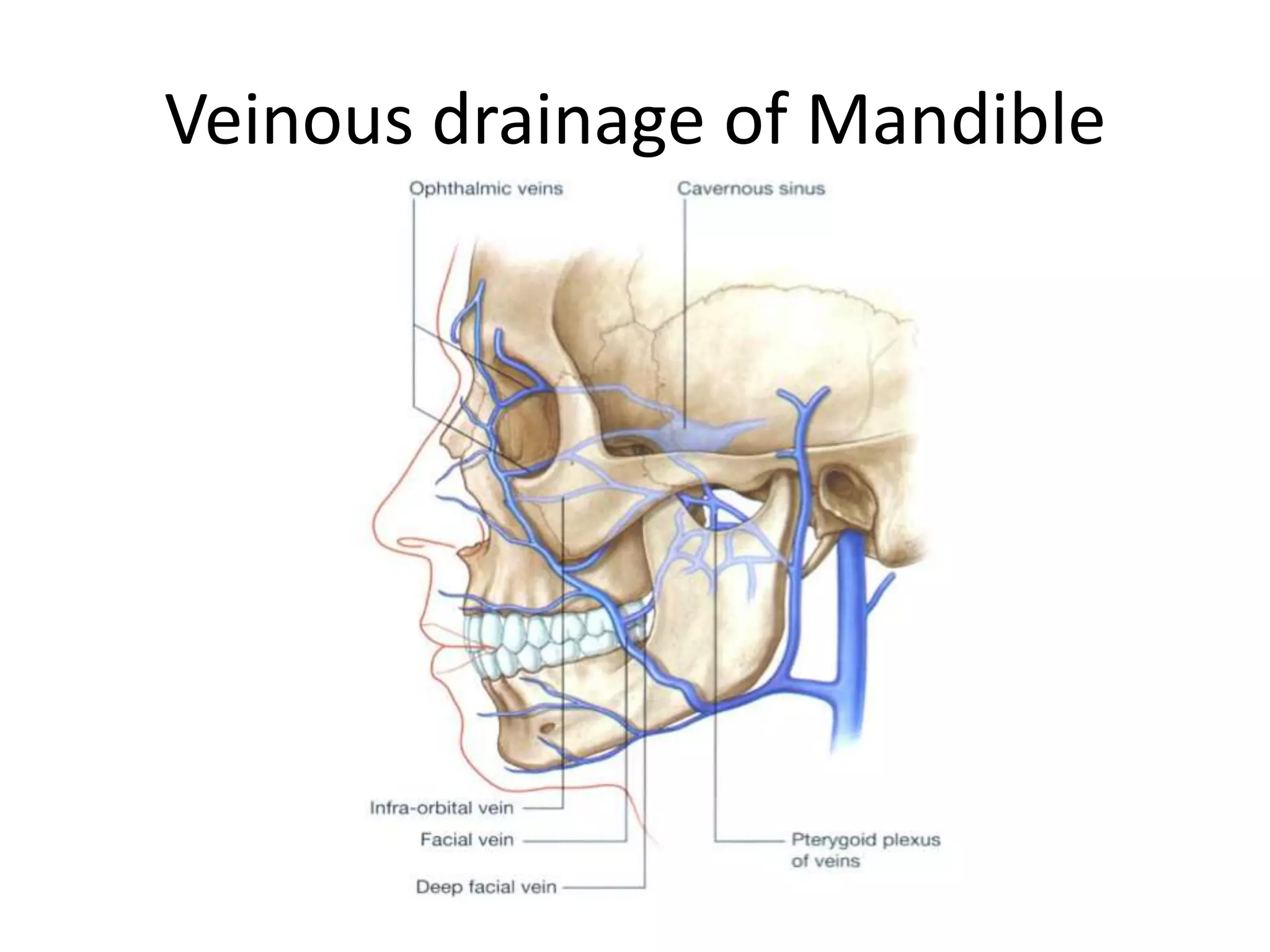
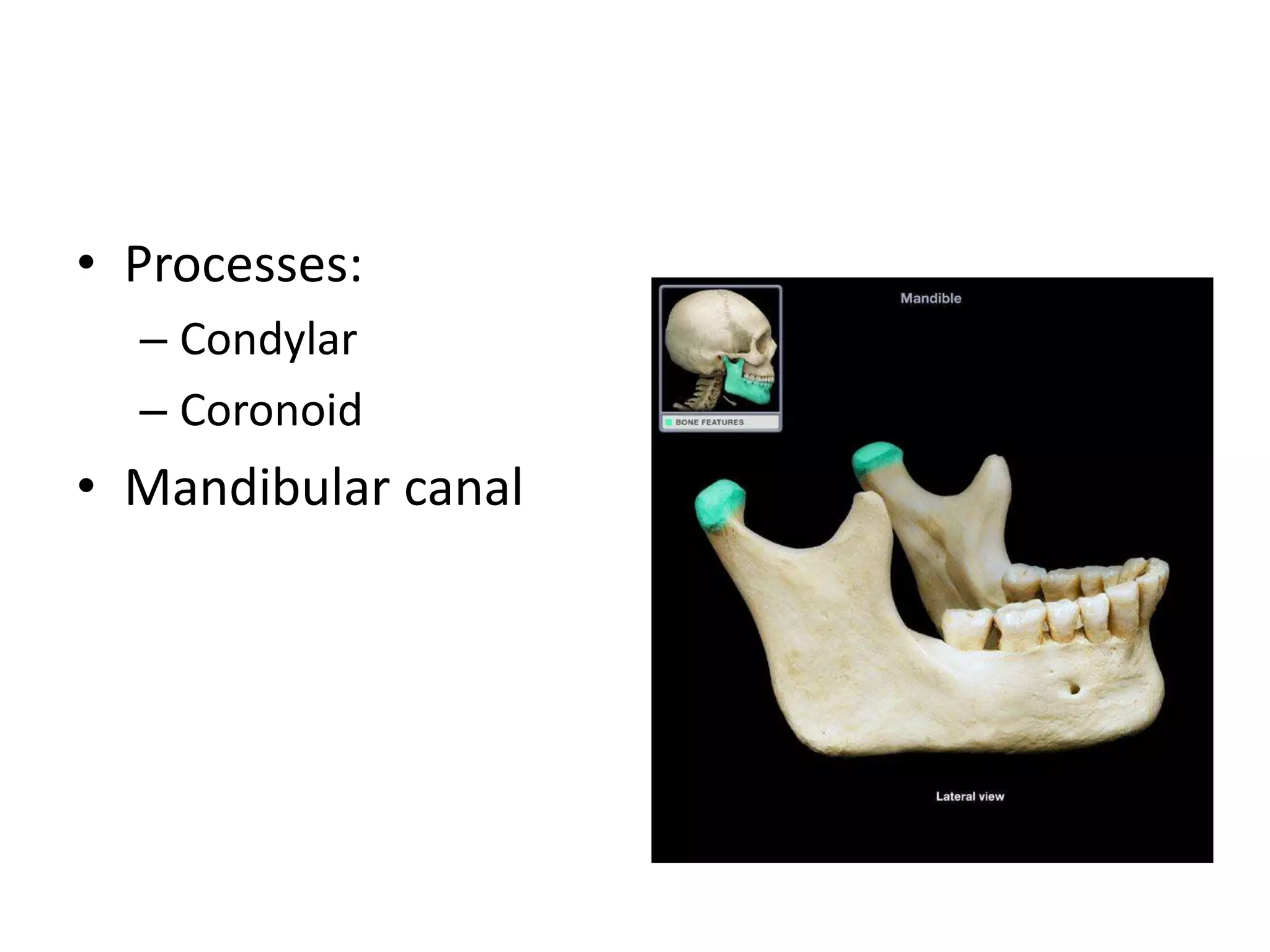
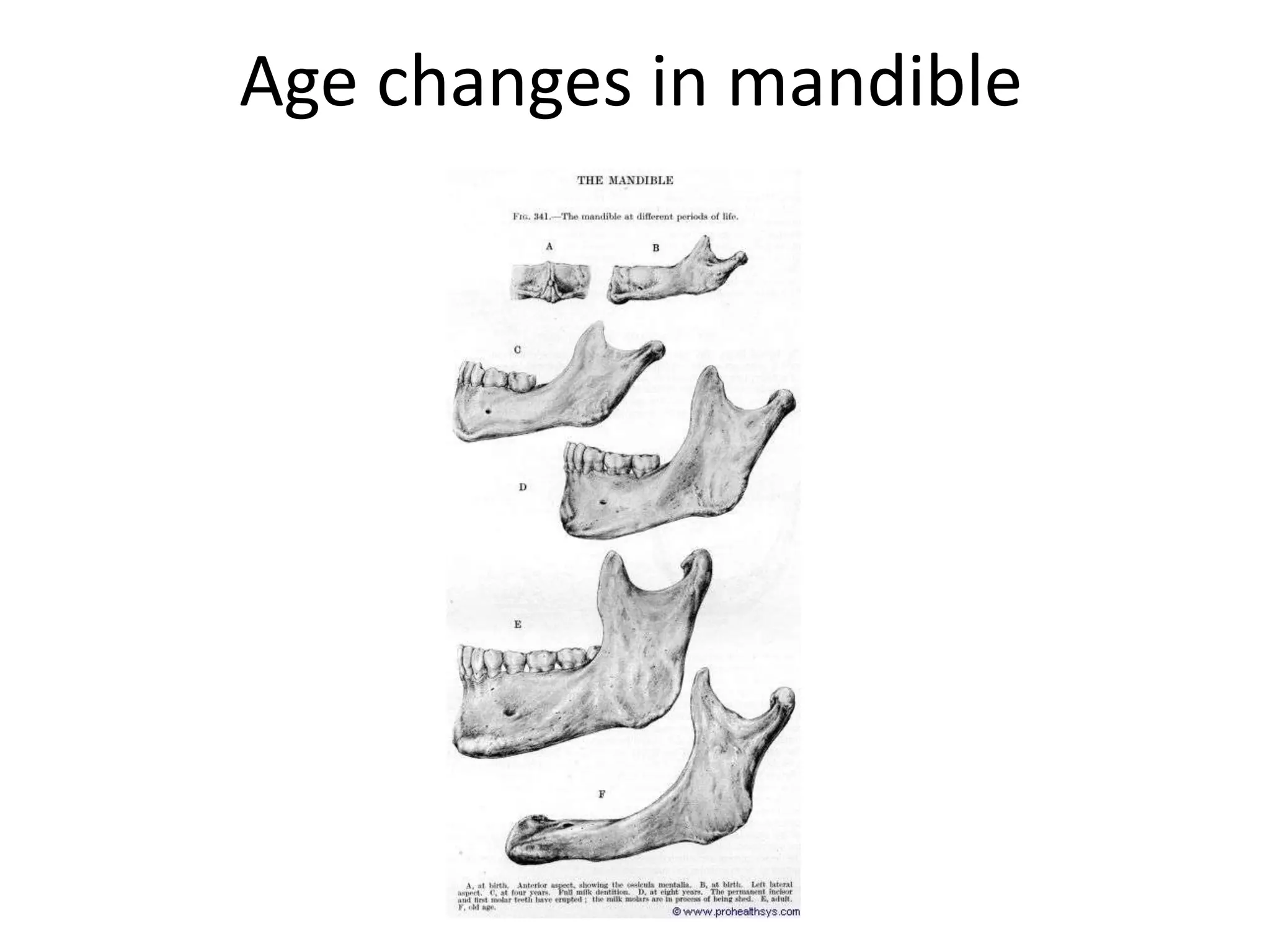


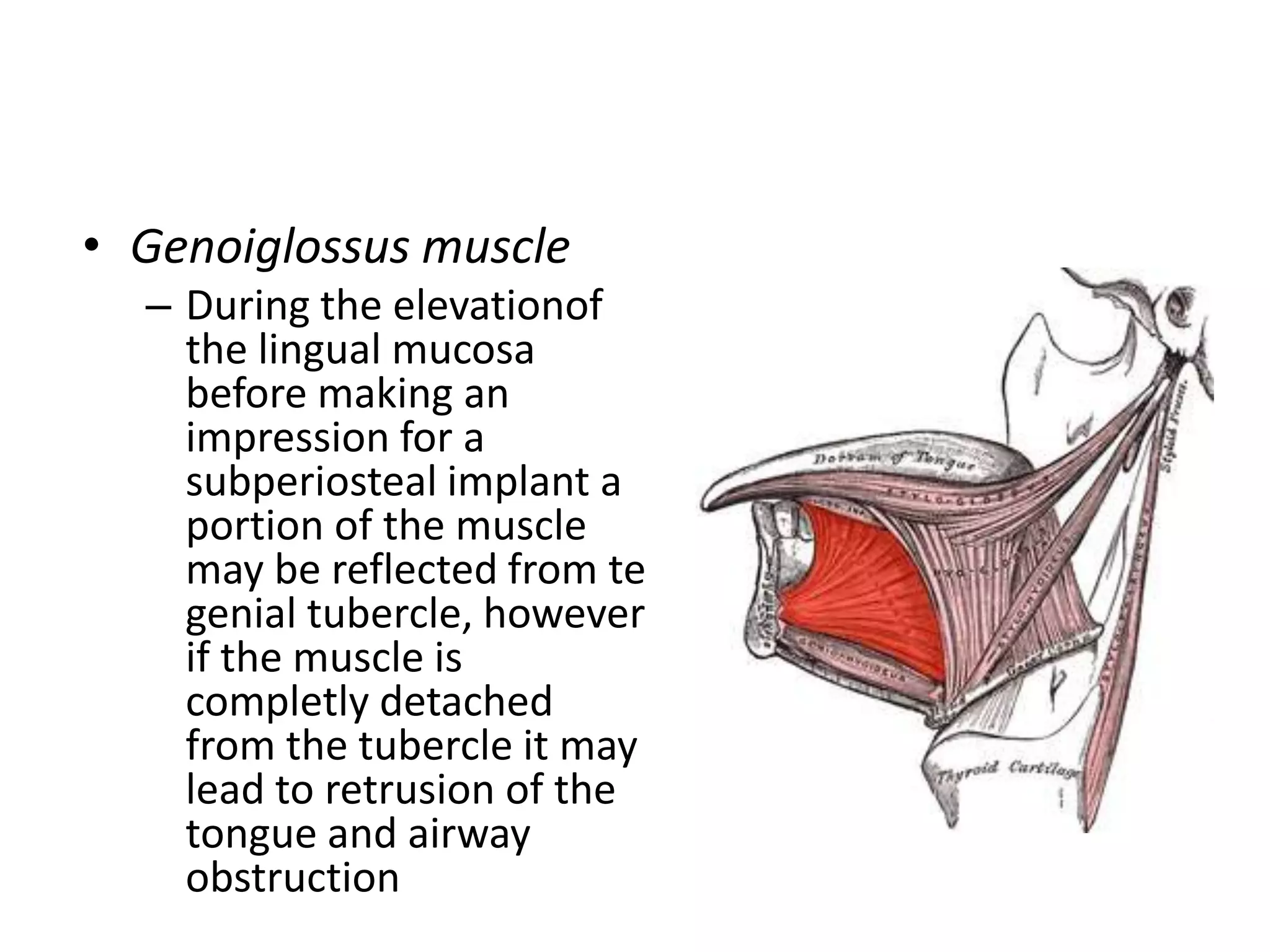
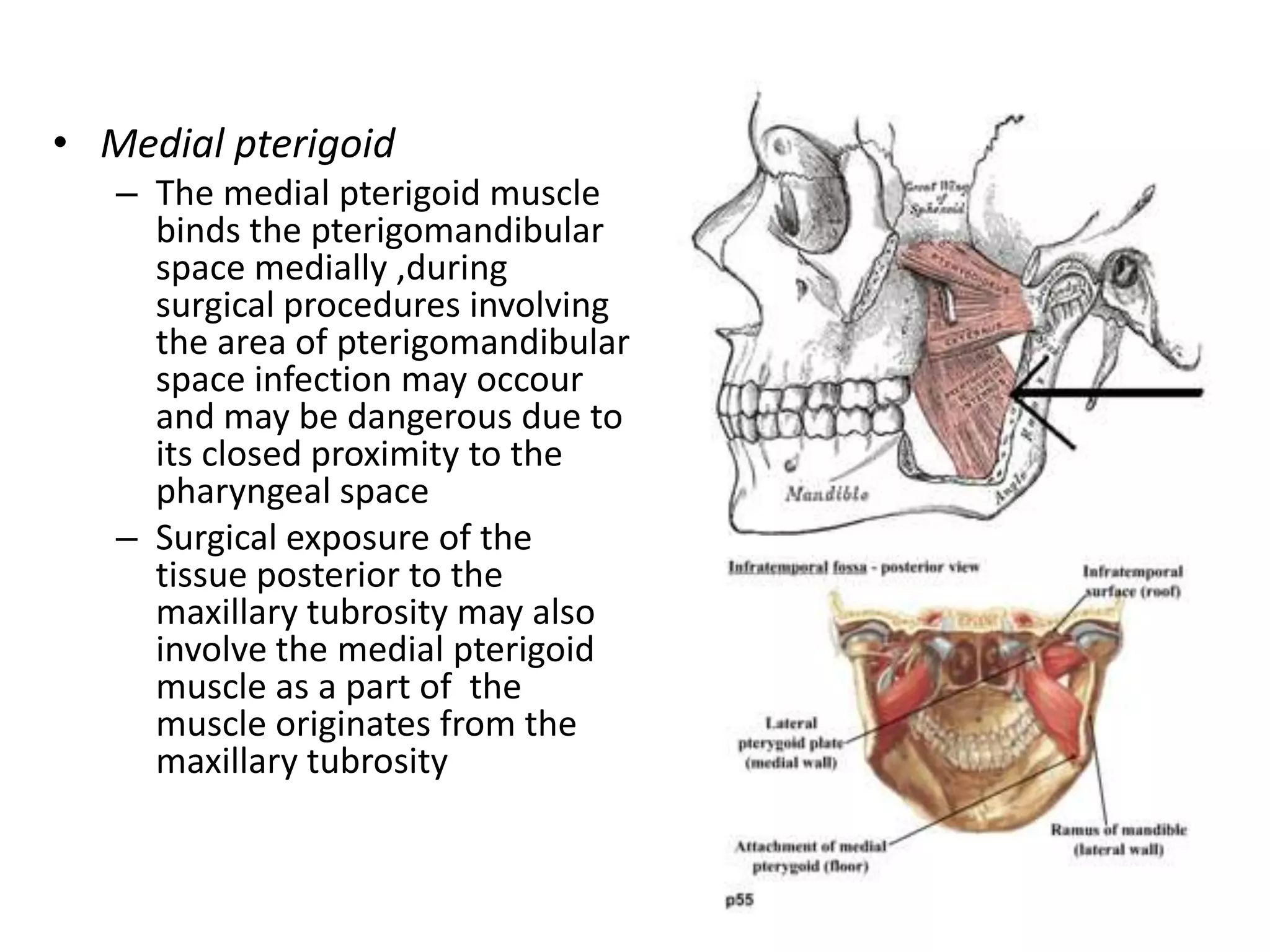


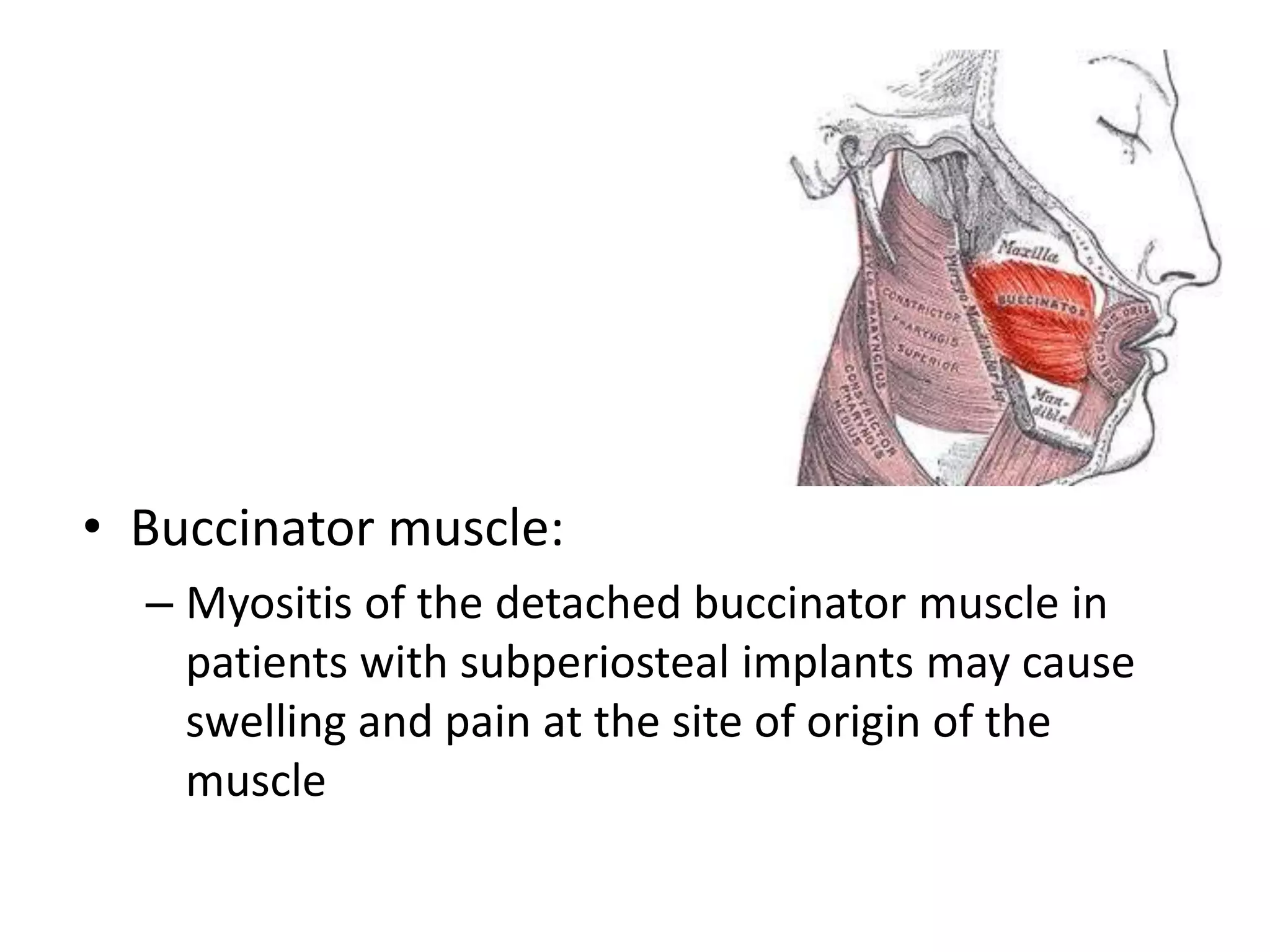


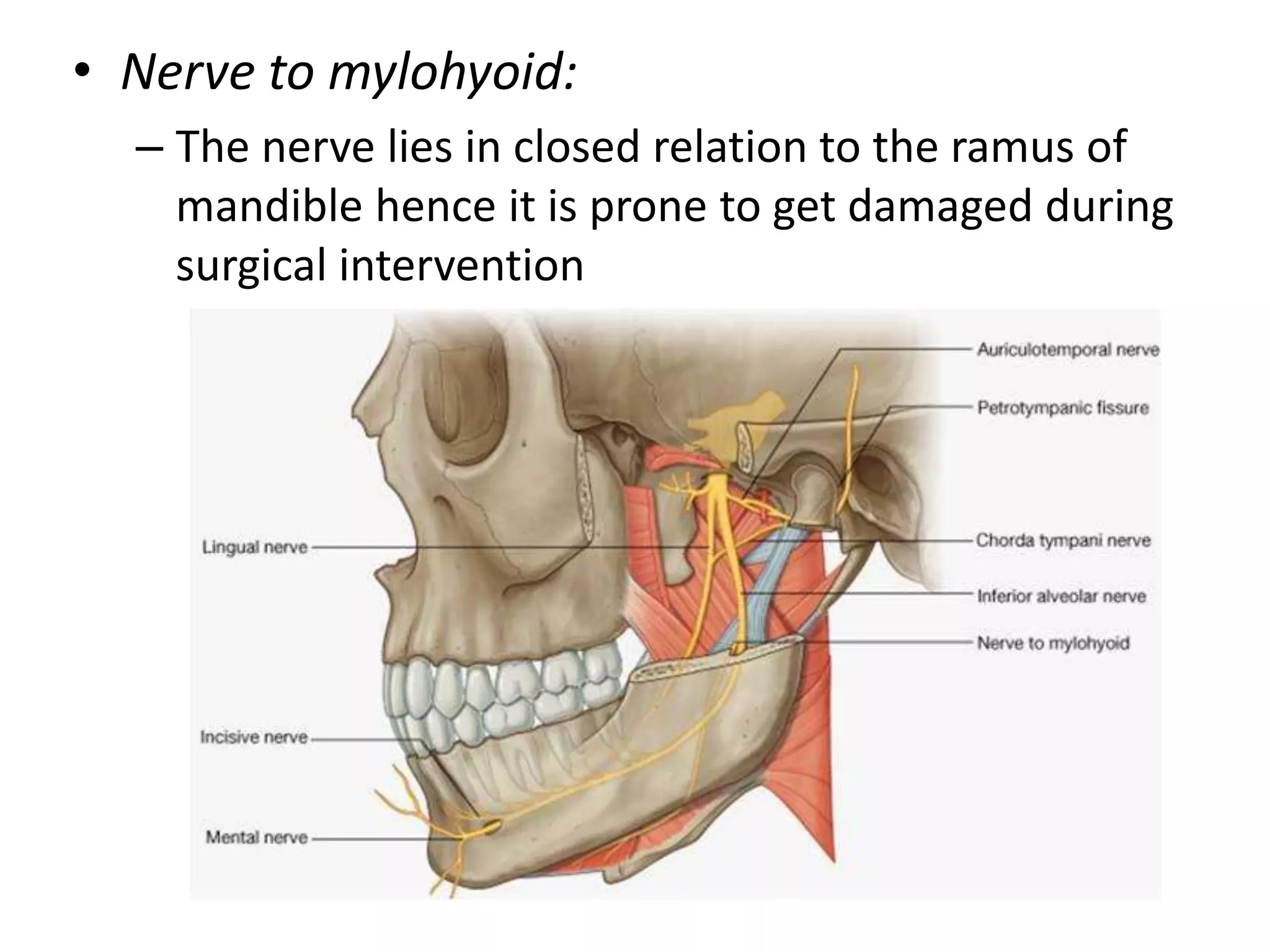

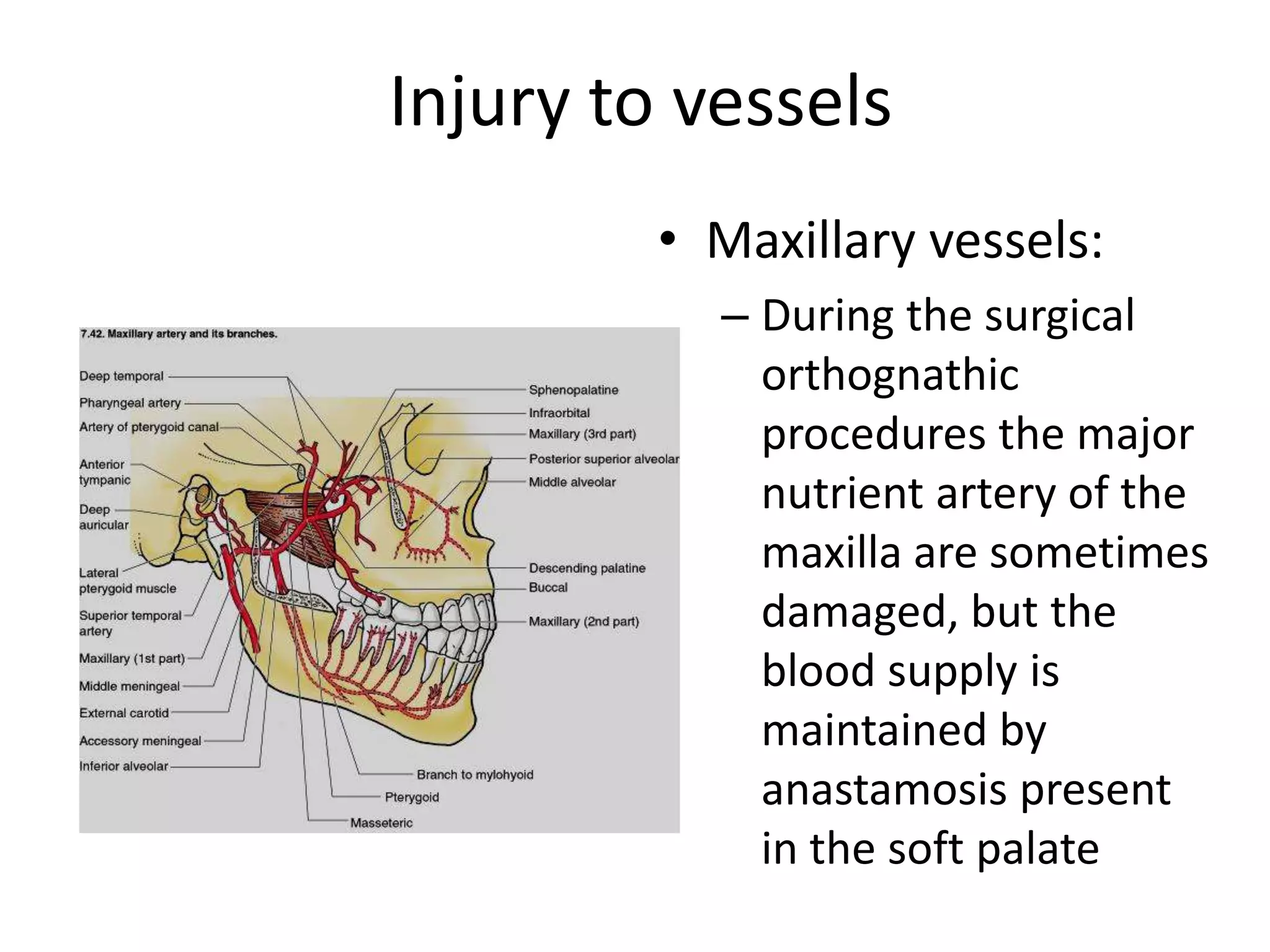


The document discusses the anatomy of the maxilla and mandible, detailing their structures, surfaces, processes, and the associated muscle and nerve considerations, particularly in relation to surgical implications. It highlights the maxilla's role as the second largest facial bone and the mandible as the largest, including their features such as foramina, processes, and the maxillary sinus. Various injuries and complications related to muscle and nerve damage during dental procedures are also addressed.

















































































