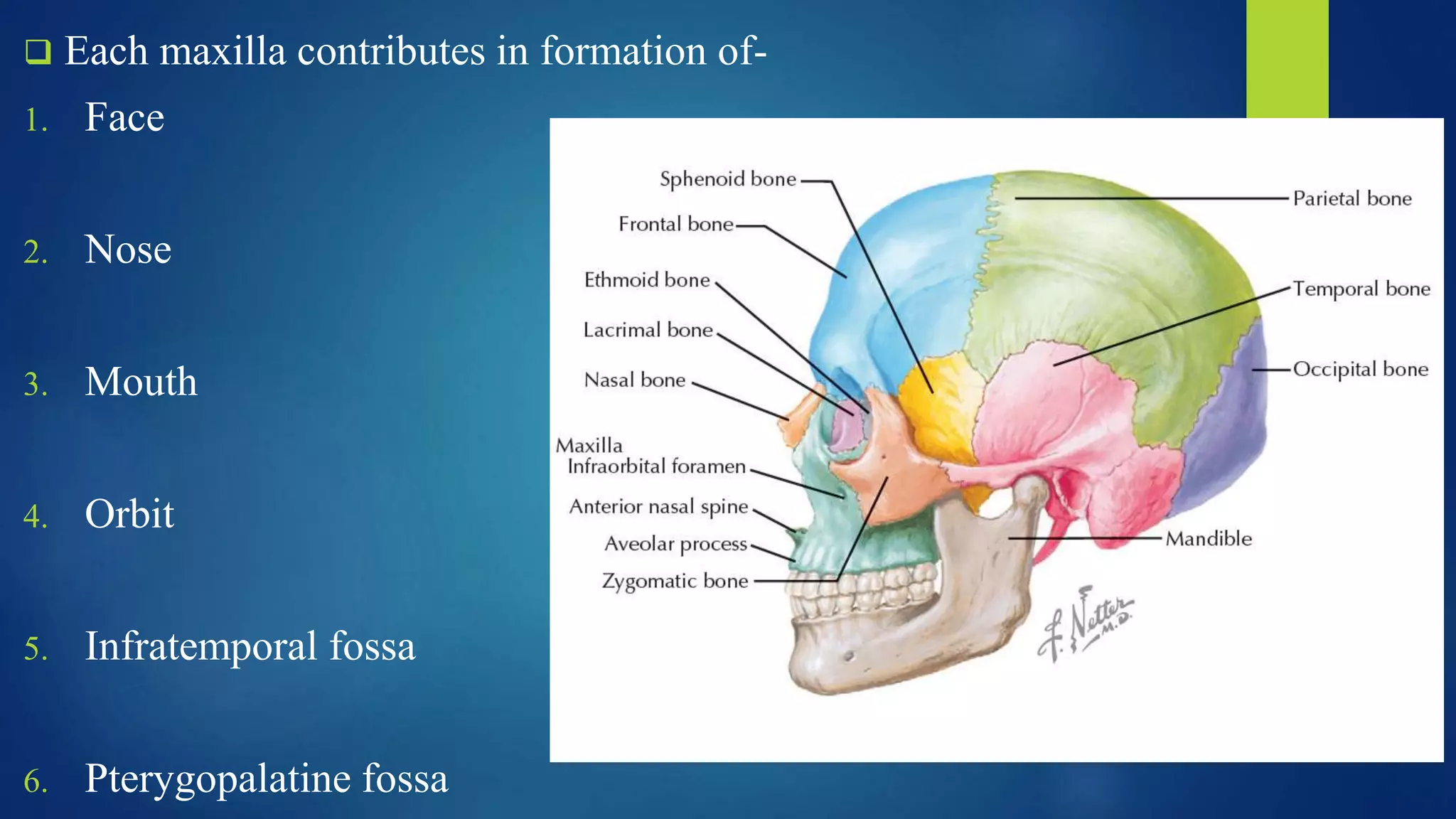
This document provides an overview of the anatomy of the maxilla bone. It begins with an introduction to the maxilla as the second largest bone of the face that forms the upper jaw. It then discusses the development of the maxilla from ossification centers. The main sections cover the features and processes of the maxilla bone, including the maxillary sinus, zygomatic process, frontal process, alveolar process and palatine process. Age-related changes to the maxilla and its articulations are also summarized. Clinical correlations regarding maxilla fractures and maxillary sinusitis are briefly mentioned.