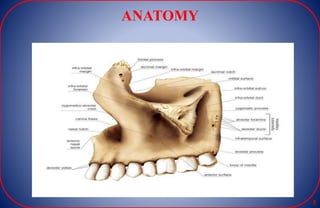
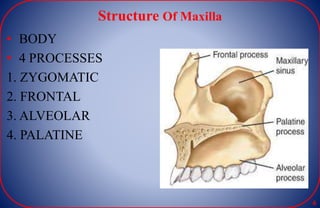
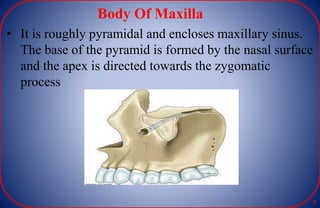
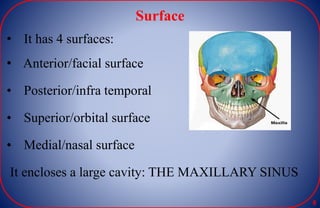
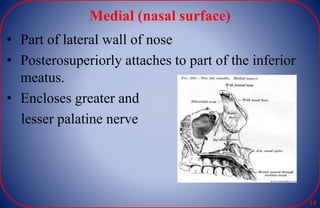
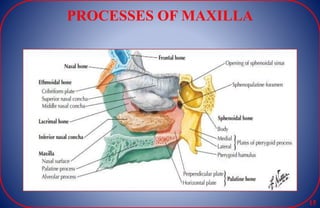
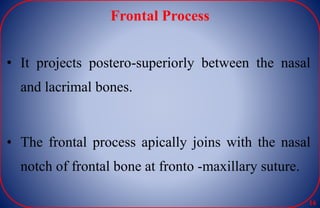
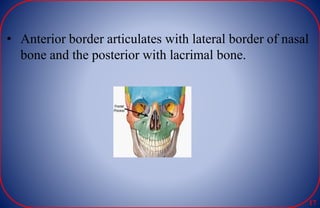
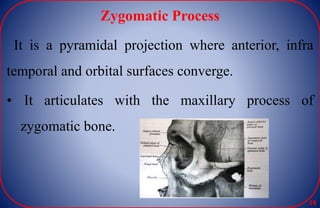
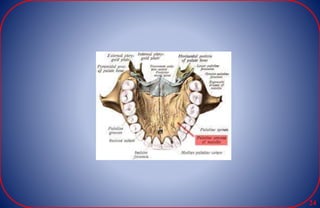
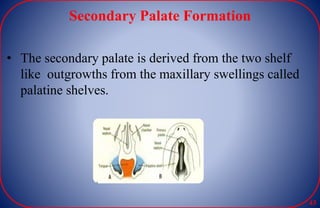
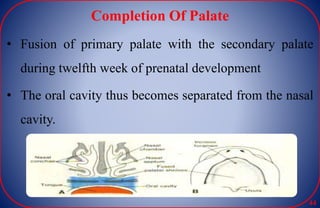
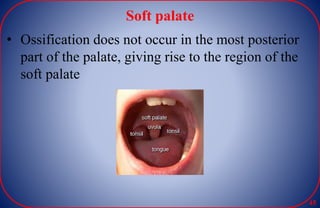
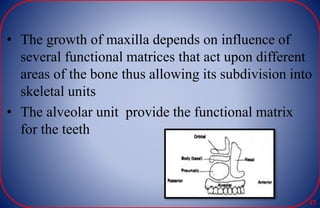
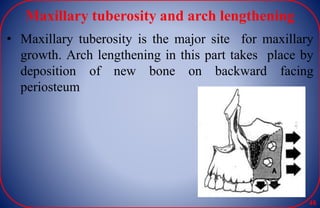
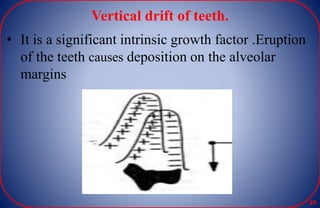
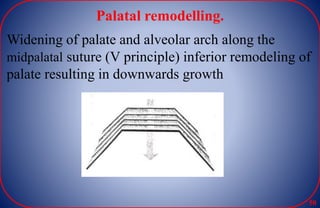
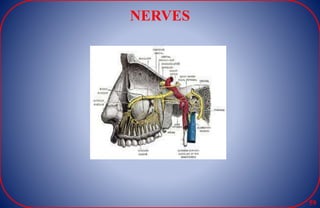
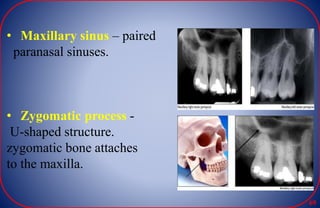
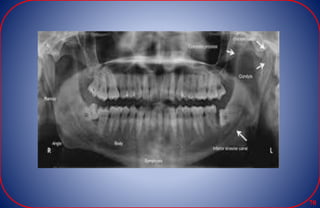
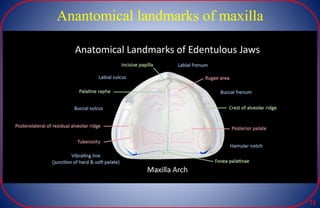
The document provides an overview of the anatomy of the maxilla bone. It discusses the structure of the maxilla including its body, processes, surfaces, and the maxillary sinus. It also covers the growth and development of the maxilla from the prenatal period through aging. Key anatomical landmarks, radiographic landmarks, nerves, vessels, and muscle attachments related to the maxilla are described.