Downloaded 486 times

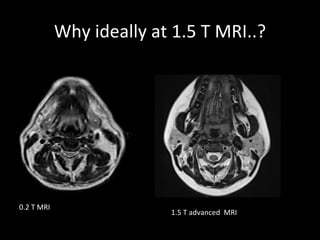
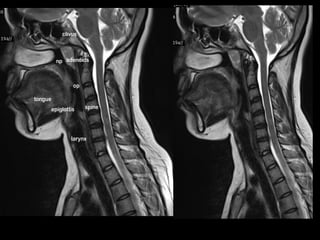
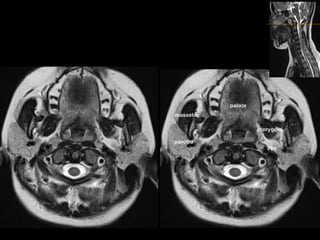

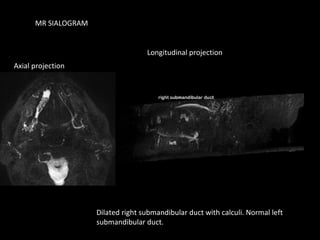
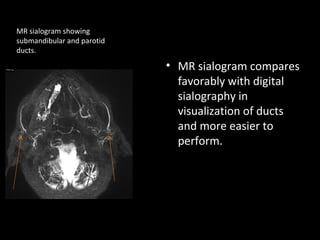
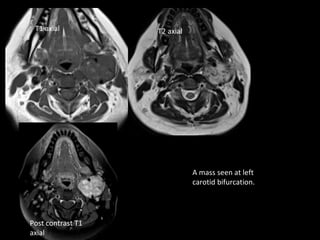
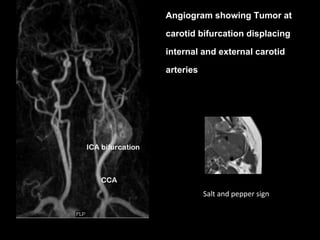
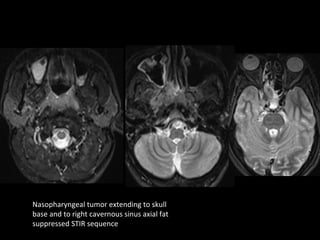
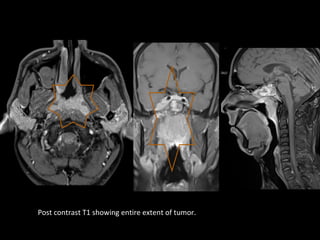
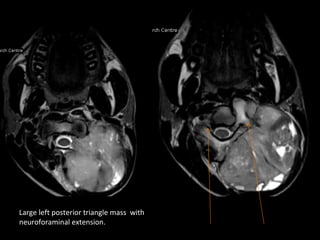
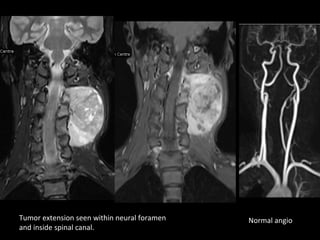


T1, T2, and fat suppressed sequences provide different contrasts in MRI neck imaging. Ideally MRI is performed at 1.5T for advanced imaging. MR sialograms compare favorably to digital sialography for visualizing salivary ducts. Carotid body tumors are hypervascular and located at the carotid bifurcation, displaying a "salt and pepper" sign. Nasopharyngeal carcinoma extends into the skull base and cavernous sinus. Neurogenic tumors can extend intraspinally. MRI is better than CT for assessing upper neck, skull base, and pediatric lesions while CT is better for lower neck and bone involvement.










![Radiological anatomy of_temporal_bone[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyoftemporalbone1-171112100915-thumbnail.jpg?width=640&height=640&fit=bounds)



















































































