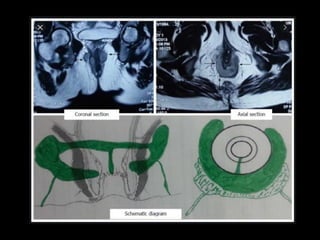
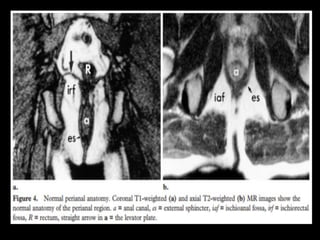
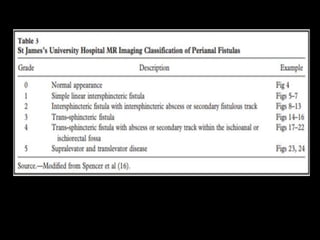
This document discusses MR imaging techniques for evaluating perianal fistulas. It begins by describing the anatomy of the perianal region and anal sphincter mechanism. It then discusses the aims and implications of MR imaging-based grading of fistulas. Various fistula classifications and types are defined based on their relationship to anal anatomy. The document outlines normal anal region anatomy as seen on MR images and techniques for identifying fistulous tracks, abscesses, and complications. It emphasizes the importance of MR imaging in surgical planning and treatment of perianal fistulas.
























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








