Downloaded 1,264 times
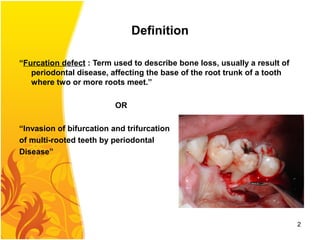
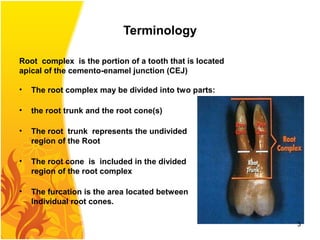
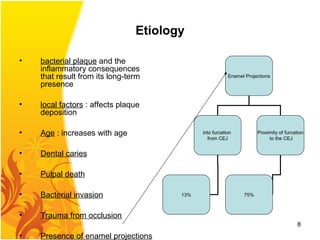
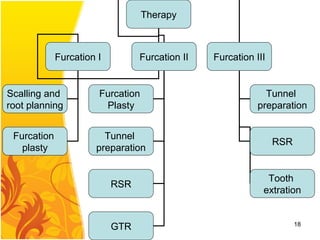

1) The document discusses furcation involvement in multi-rooted teeth due to periodontal disease. It defines furcation defects and provides terminology to describe root anatomy involved in furcation defects. 2) Classification systems for furcation defects from Hamp and Glickman are presented, ranging from initial horizontal bone loss to complete bone loss exposing the furcation. 3) Diagnosis and treatment options for different degrees of furcation involvement are outlined, including furcation plasty, tunnel preparation, root separation/resection, guided tissue regeneration, and extraction.









































































































