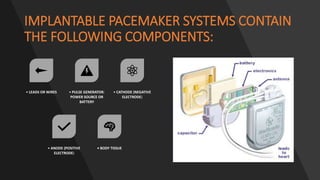
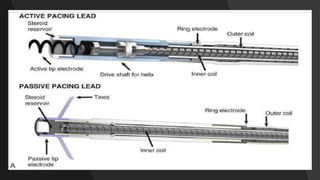
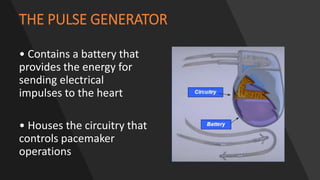
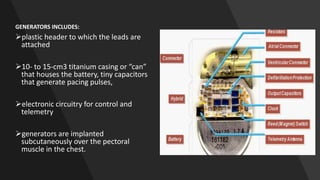
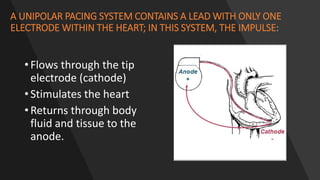
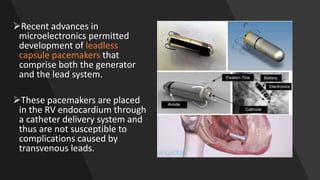
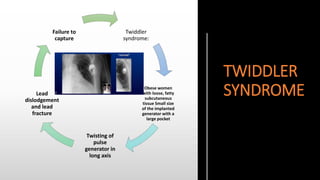
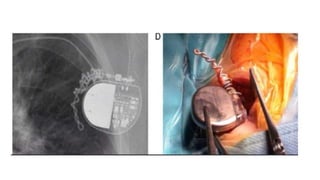
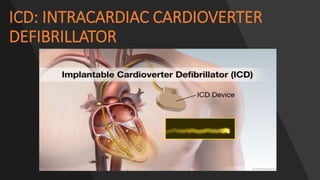
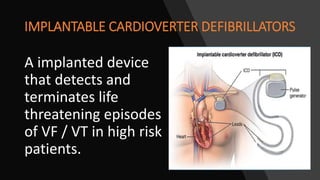
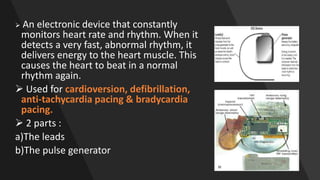
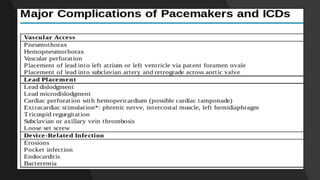
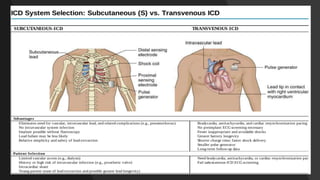
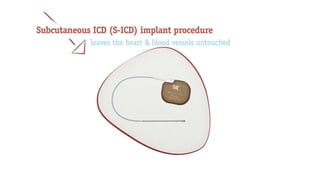
This document discusses intracardiac devices such as pacemakers and implantable cardioverter defibrillators (ICDs) and their components and complications. Pacemakers and ICDs contain leads that deliver electrical pulses to the heart from a pulse generator containing a battery and circuitry. Pacemakers treat bradycardia with low-voltage pulses while ICDs treat ventricular fibrillation and tachycardia with high-voltage shocks. Complications can include lead dislodgement, infection, and device malfunctions. Permanent pacemaker implantation is indicated for symptomatic bradycardia and heart block depending on severity and symptoms. ICDs are implanted in patients at high risk of life-threatening arrhythm








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






