3. Case Presentation
• CC: Melena
• HPI: 54 yo man taking ibuprofen 200
mg po tid for the past 2 wks b/o acute
LBP after lifting presents with 2 day h/o
melena
• PMHx: neg All: NKDA SHx/FHx: neg
• Vitals: BP 105/75 P 90
• PE: normal
4. Clinical Presentation
Hematemesis: bloody vomitus (bright red or
coffee-grounds)
Melena: black, tarry, foul-smelling stool
Hematochezia: bright red or maroon blood
per rectum
Occult: positive guaiac test
Symptoms of anemia: angina, dyspnea, or
lightheadedness
5. Patient Assessment
• Hemodynamic status
• Localization of bleeding source
• CBC, PT, and T & C
• Risk factors
– Prior h/o PUD or bleeding
– Cirrhosis
– Coagulopathy
– ASA or NSAID’s
6. Resuscitation
• 2 large bore peripheral IV’s
• Normal saline or LR
• Packed RBCs
• Correct coagulopathy
7. Location of Bleeding
• Upper
– Proximal to Ligament of Treitz
– Melena (100-200 cc of blood)
– Azotemia
– Nasogatric aspirate
• Lower
– Distal to Ligament of Treitz
– Hematochezia
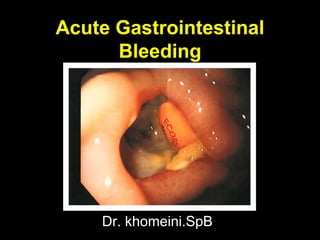
8. Acute UGIB
Demographics
• 10,000 - 20,000 deaths annually
• Mortality stable at 10%
• 80% self-limited
• Continued or recurrent bleeding -
mortality 30-40%
9. • Cause of bleeding
• Severity of initial bleed
• Age of the patient
• Comorbid conditions
• Onset of bleeding during
hospitalization
Acute UGIB
Prognostic Indicators
13. DIAGNOSES % OF TOTAL
Duodenal ulcer 24
Gastric erosions 23
Gastric ulcer 21
Varices 10
Mallory-Weiss tear 7
Esophagitis 6
Acute UGIB
Final Diagnoses of the Cause in 2225 Patients
Tedesco et al. ASGE Bleeding Survey. Gastro Endo. 1981.
14. DIAGNOSES % OF TOTAL
Peptic ulcer 55
Varices 14
Angioma 6
Mallory-Weiss tear 5
Erosions 4
Tumor 4
Acute UGIB
Causes in CURE Hemostasis Studies (n=948)
Savides et al. Endoscopy 1996;28:244-8.
15. Acute UGIB
CORI Database
University, VA, & private
practices
20 months (12/99-7/01)
7822 EGDs for UGIB
BoonpongmaneeS. et al. Gastrointest Endosc 2004;59:788-94.
21. Bleeding PUD: IV H2RAs
Meta-Analysis
• Duodenal ulcer: no
benefit
• Gastric ulcer: mild
benefit
– Mortality
• ARR 3%; NNT 33
– Surgery
• ARR 7%; NNT 14
– Rebleeding
• ARR 7%; NNT 14
• Caveats
– Tolerance develops
within 24 hrs
– More potent acid
suppression
available
Levine JE et al. Aliment Pharmacol Ther 2002;16:1137-42.
22. 472 patients required no
endoscopic treatment
27 patients not included:
comorbid or no consent
120 patients received IV
omeprazole 80 mg bolus
then 8 mg/hr for 72 hours
120 patients received placebo
267 received endoscopic treatment
739 patients admitted with GI bleeding
Lau et al. New Eng J Med 2000;343:310-316.
Adjuvant Medical Therapy of
PUD
24. Bleeding PUD: PO/IV PPIs
Meta-Analysis
• Reduction in:
– Rebleeding NNT* 4-17
– Surgery NNT* 6-25
• No change in mortality
• PPIs add to endoscopic
therapy but do not
supplant endoscopic
therapy
* Estimates from pooled ORs
Leontiadis, GI et al. BMJ 2005;330:568-75.
34. Case Presentation
• CC: Hematochezia
• HPI: 74 yo woman presents with 6 hour
history of painless maroon blood per rectum
• PMHx: CAD, Chol, AFib, CABG, L-CEA
• Meds: ASA, coumadin, digoxin, lovastatin
• Vitals: BP 105/75 P 90
• PE: irreg rhythm, maroon blood on DRE
40. Urgent Colonoscopy for the Diagnosis
and Treatment of Severe Diverticular
Hemorrhage
• 121 pts with severe
bleeding (>4 hrs
after hospitalization)
• 1st 73 pts: no
colonoscopic tx
• Last 48 pts eligible
for colonoscopic tx
• Colonoscopy w/in 6-
12 hrs
41. Urgent Colonoscopy for the Diagnosis and
Treatment of Severe Diverticular
Hemorrhage
Jensen DM, et al. New Eng J Med 2000:342:78-82.