Downloaded 291 times
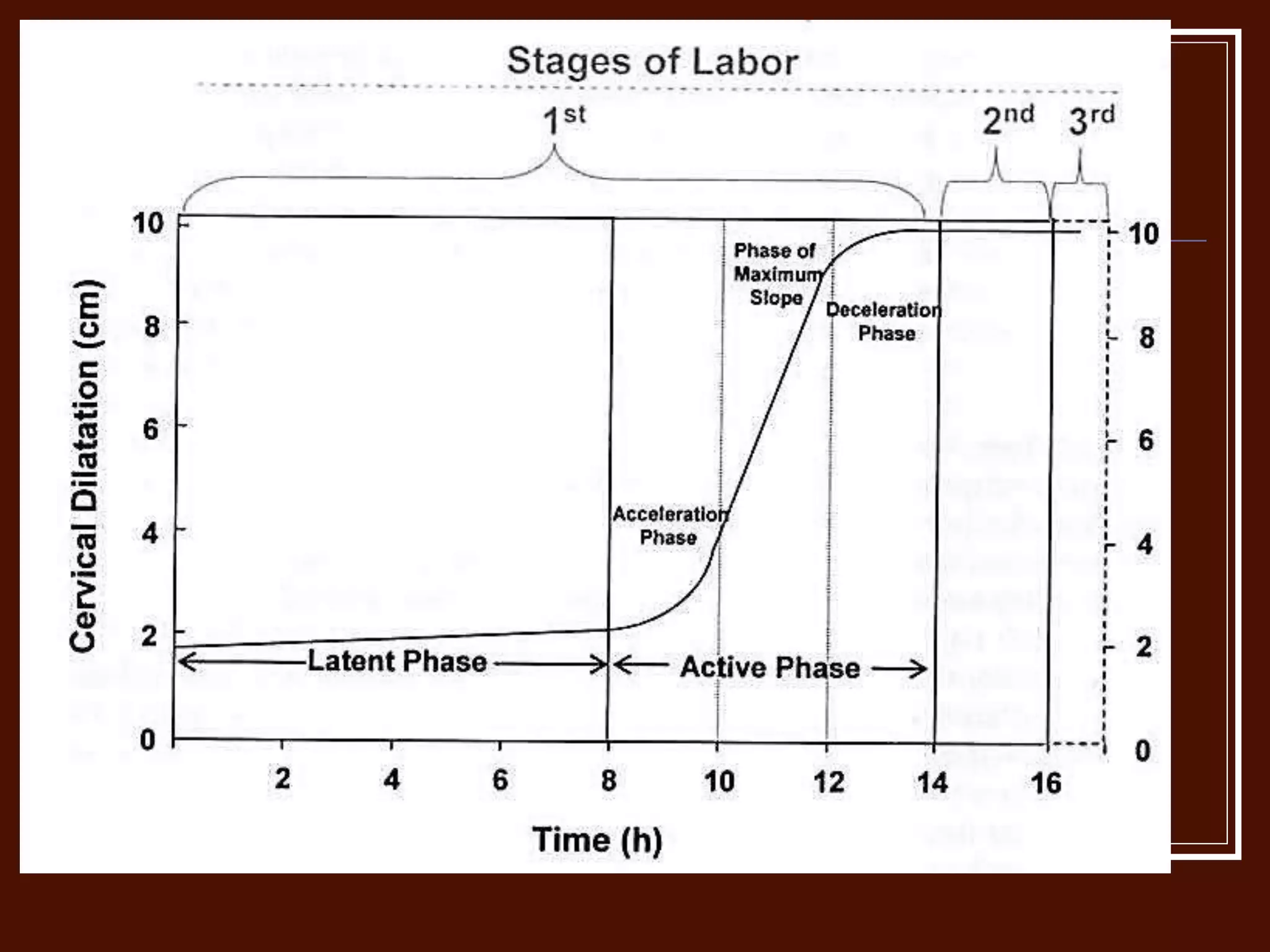
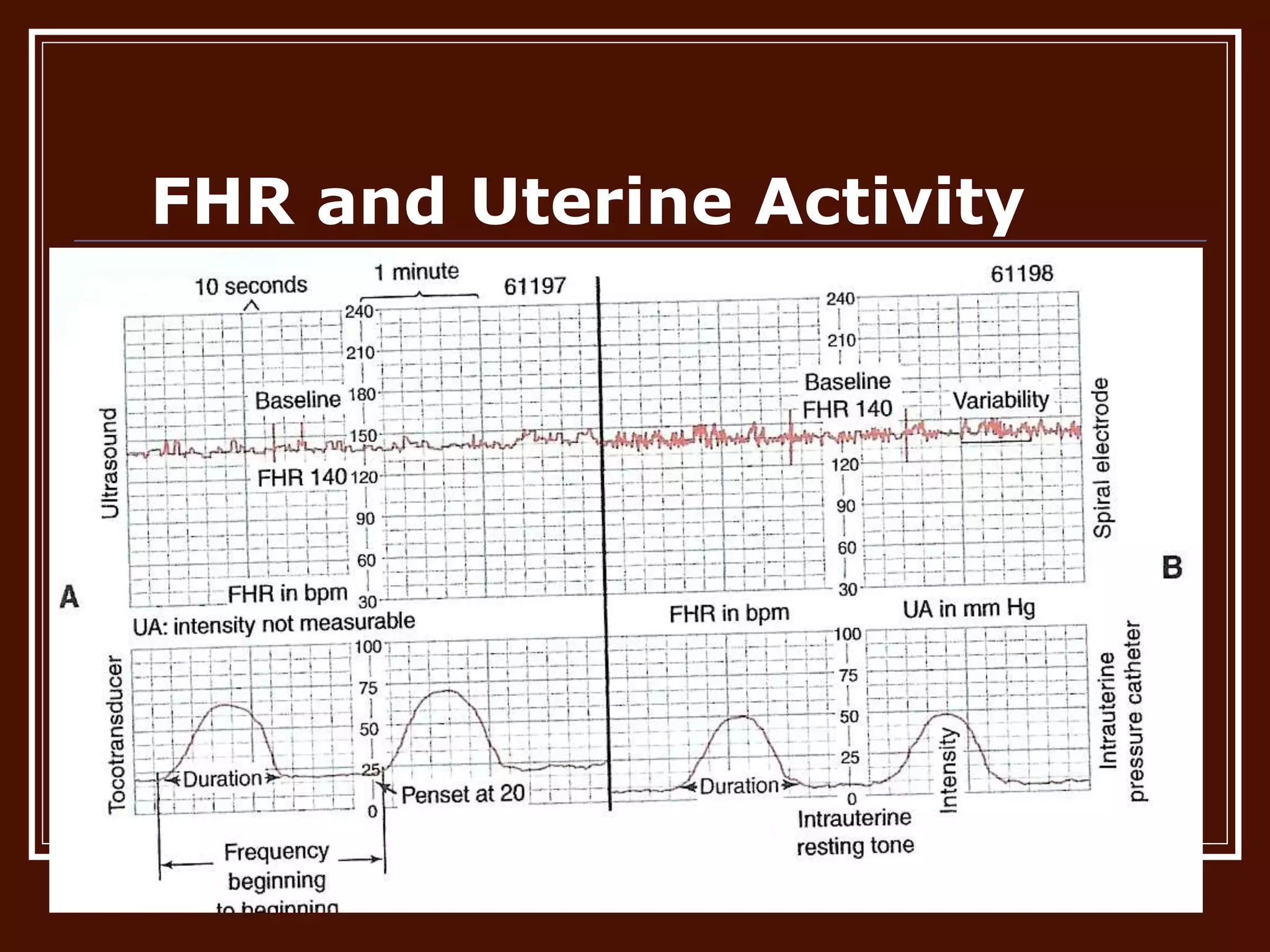

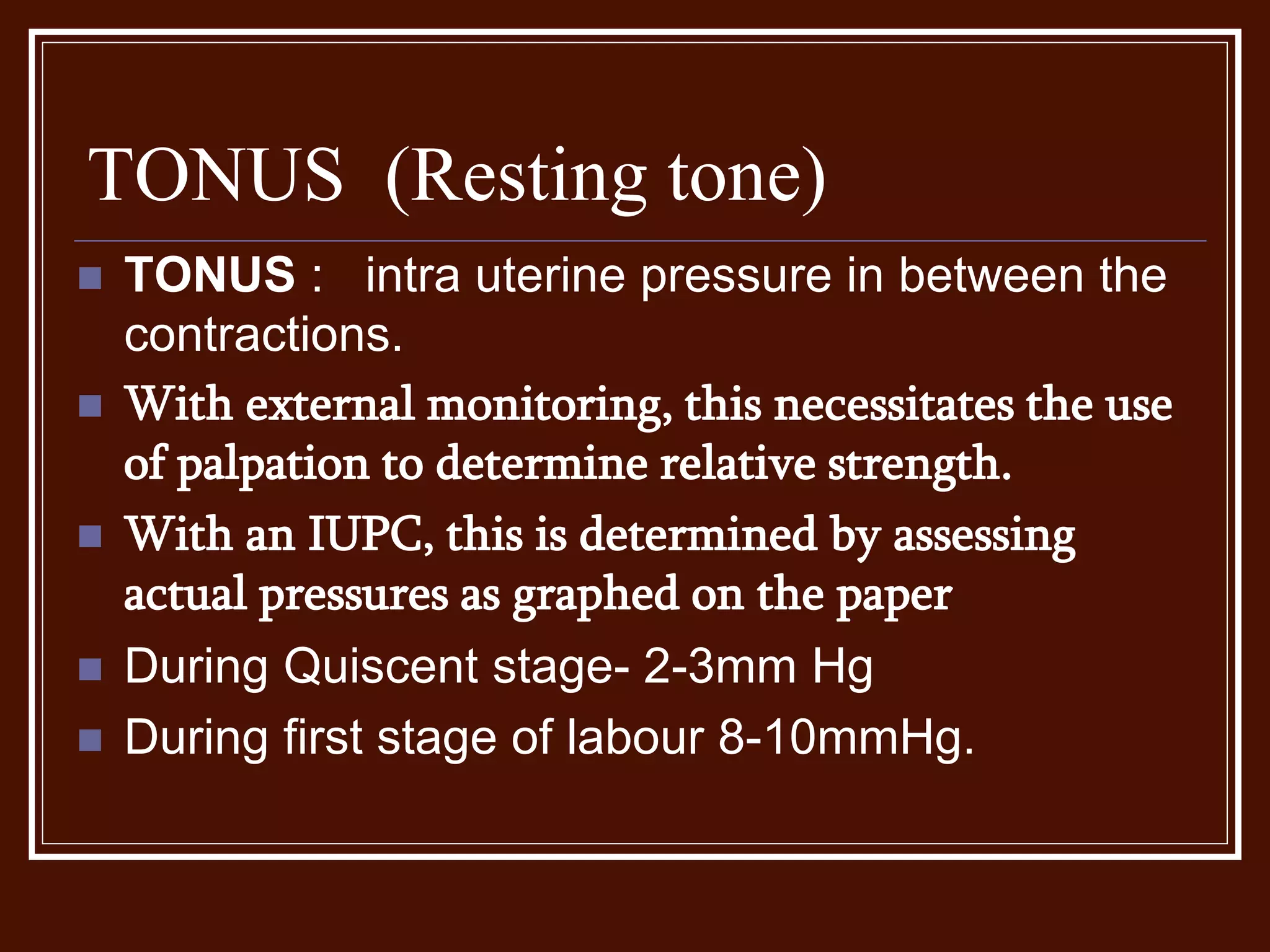
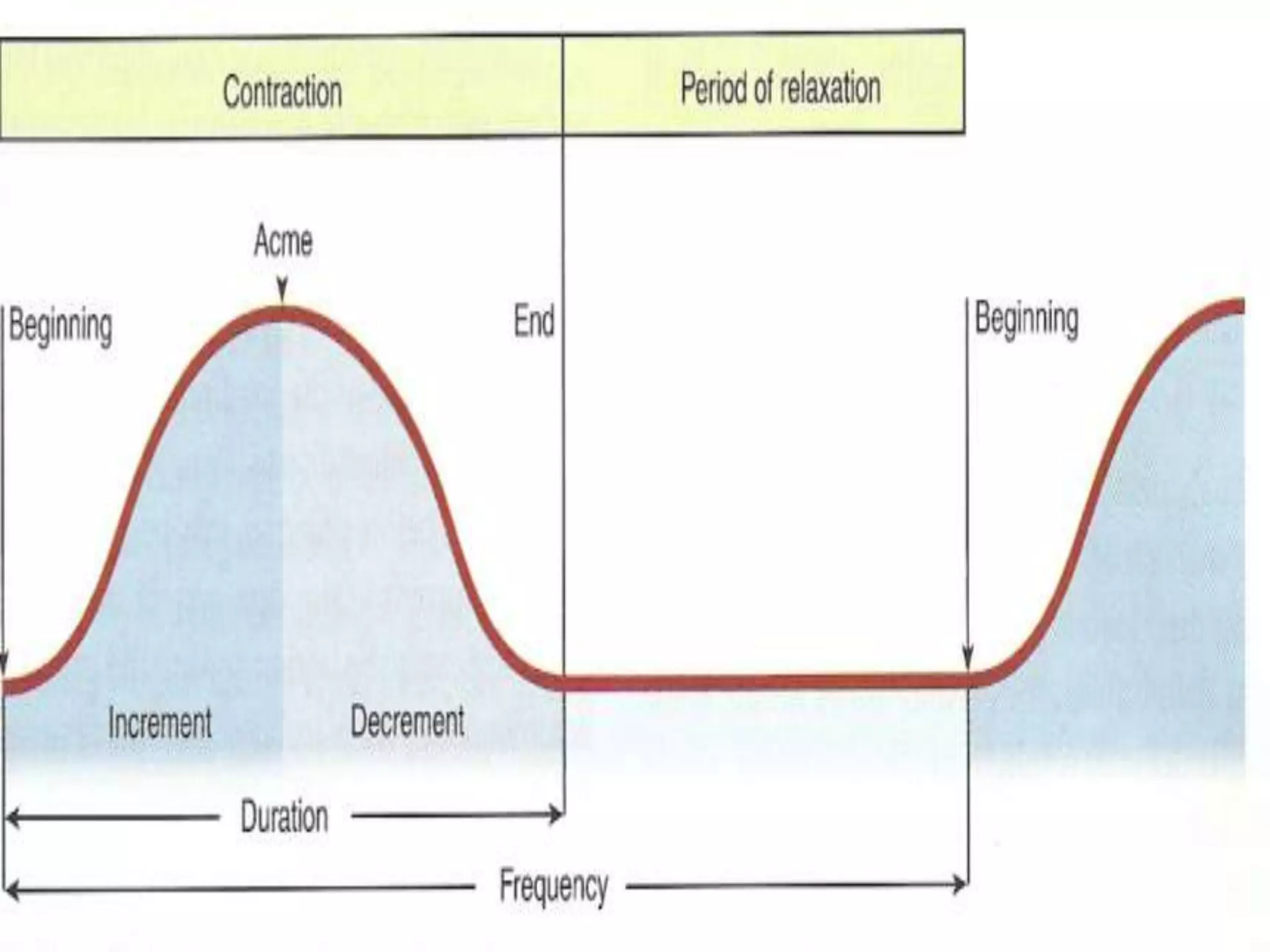
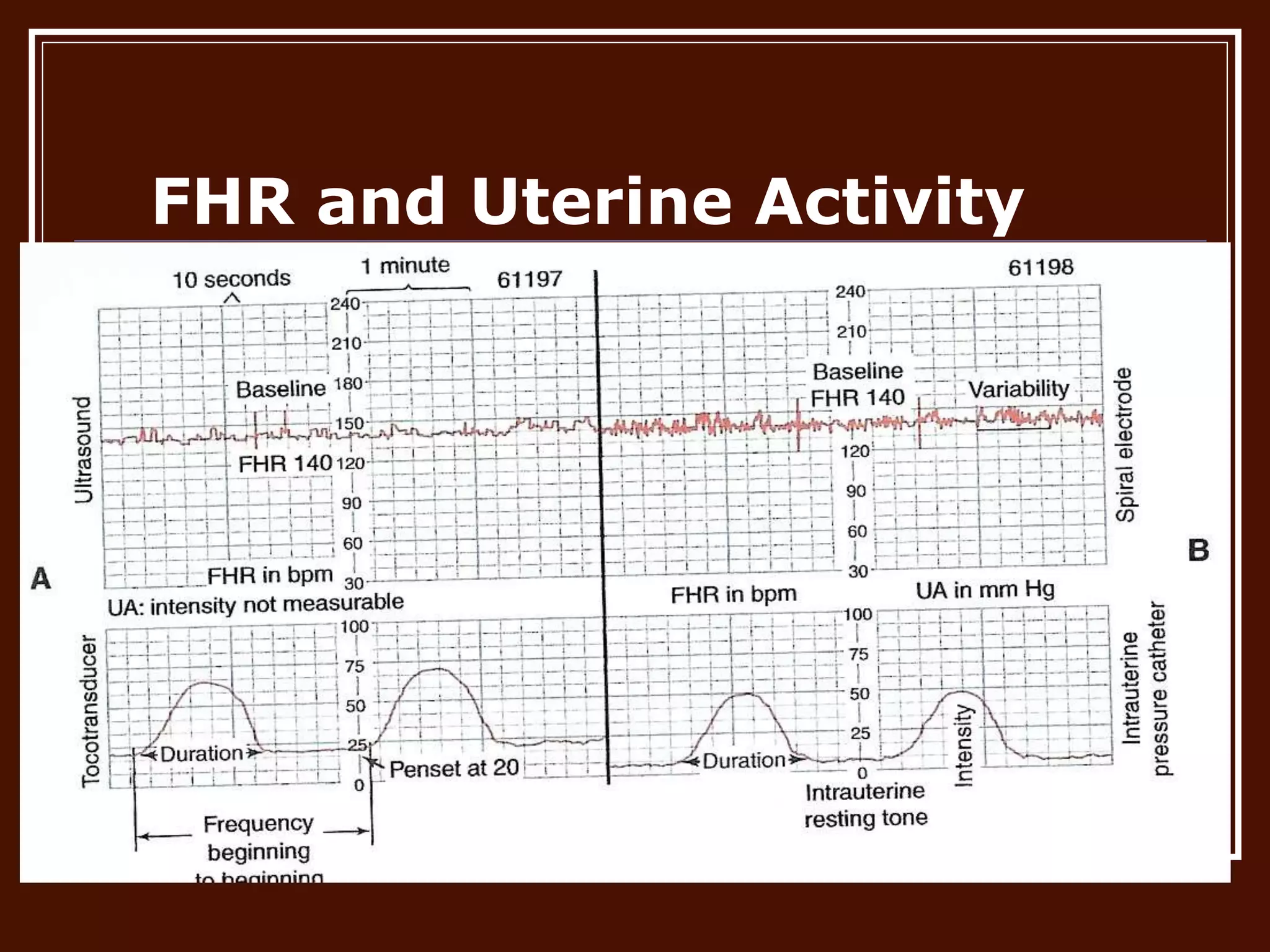


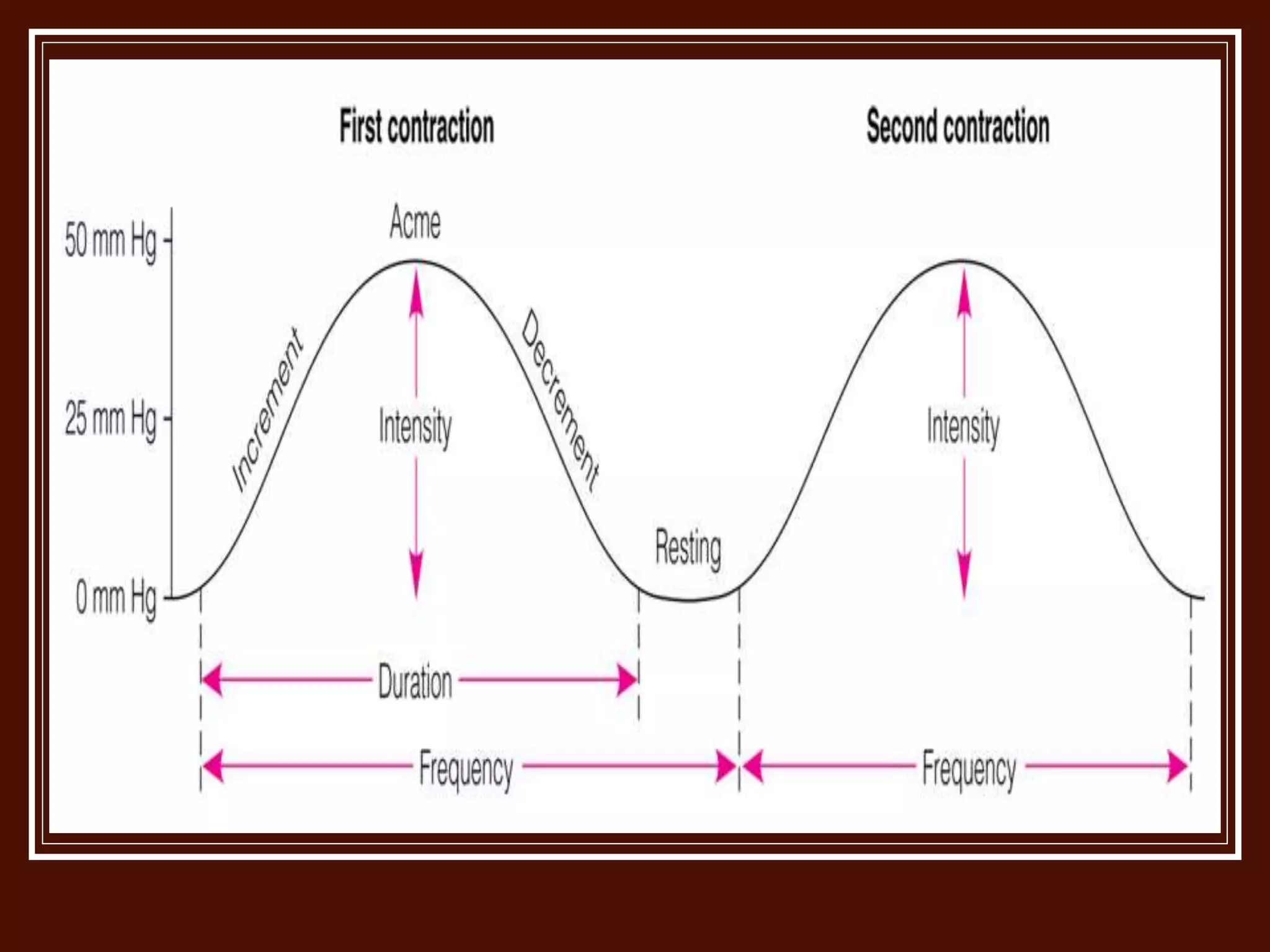




This document discusses normal uterine action during labor, which comprises 4 stages: 1) cervical dilation, 2) delivery of the baby, 3) placental separation and expulsion, and 4) the first hour after delivery. It describes the major events during labor like increasing contractions, cervical effacement and dilation. Contraction characteristics like frequency, duration, intensity, and resting tone are defined. Abnormal uterine contractions can cause ineffective labor and are classified as coordinated issues like hyperfunction or hypofunction, or incoordinated issues like a colicky or tonic uterus.












































































