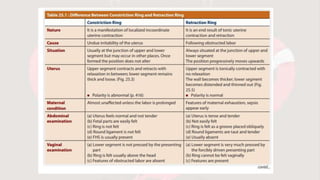
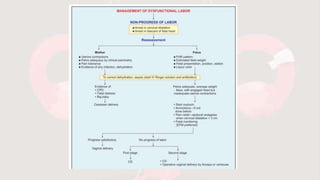
This document summarizes various types of abnormal uterine action that can occur during labor and delivery. It describes normal labor progression and defines abnormalities as any deviation from the normal pattern of uterine contractions that affects the course of labor. Various types of abnormalities are outlined, including dysfunctional labor, uterine inertia, incoordinate uterine action, cervical dystocia, and precipitate labor. Causes, diagnostic features, effects on the mother and fetus, and management approaches are provided for each abnormality.












































![DYSFUNCTIONAL UTERINE ACTION [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dysfunctionaluterineactionautosaved-250728183222-c94b3c6b-thumbnail.jpg?width=640&height=640&fit=bounds)


























