
Downloaded 816 times



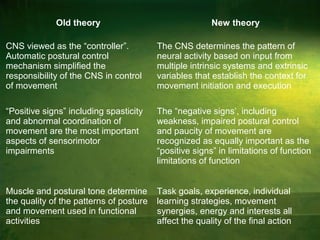
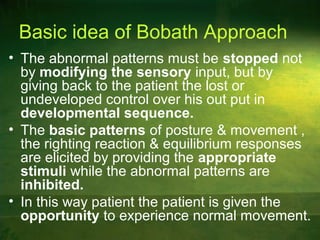
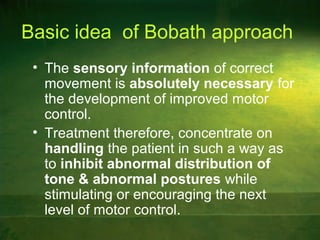
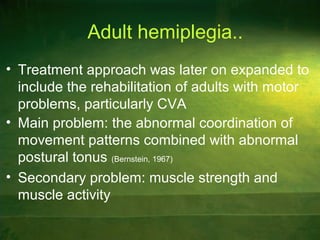






This document discusses the Bobath and Brunnstrom approaches to neurodevelopmental therapy, outlining their theoretical bases and treatment principles. It elaborates on motor control systems, the significance of reflexes, and the importance of facilitating normal patterns of movement while inhibiting abnormal ones in patients with hemiplegia and cerebral palsy. Key points of control and treatment techniques are also presented, emphasizing a holistic approach to rehabilitation.












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










