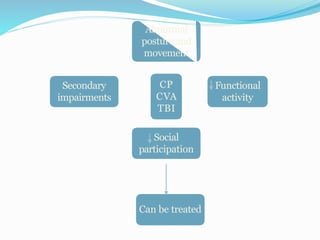
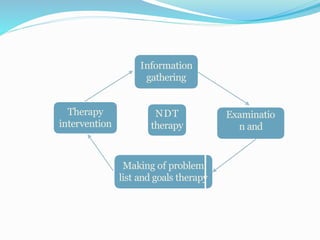
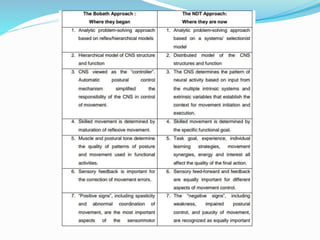
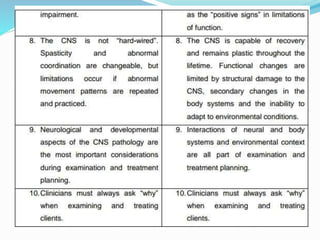
The document outlines the principles and practices of the Neuro-Developmental Treatment (NDT) approach, originally developed by Berta and Karel Bobath, which focuses on the assessment and treatment of movement and posture dysfunctions in individuals with neurological conditions. It emphasizes the role of neuroplasticity in regaining motor control and the importance of involving the patient and family in the therapeutic process. The document also details various strategies and assessments that can be employed to optimize functional outcomes in therapy.