Downloaded 38 times
![Mx
• Non - operative – PHYSIOTHERAPY
• Operative Mx
- a} Anterior instability-
key factors- < 20yrs
- activity of the person
[sports person , active military
personal,climbers]
- pts expectations](https://image.slidesharecdn.com/currentconceptsinthemanagementofshoulderinstability-180922111952/75/Current-concepts-in-the-management-of-shoulder-instability-14-2048.jpg)
![• In instability due to large Hill- Sachs lesion,
there is a role for arthroscopic reimplissage
procedure [ French to fill up]
• This involves using the capsule & infraspinatus
to fill up a large engaging Hill- Sachs defect
usually in combination with anterior bankart
repair.
• It makes the defect extrarticular so that it
does not engage against glenoid edge](https://image.slidesharecdn.com/currentconceptsinthemanagementofshoulderinstability-180922111952/75/Current-concepts-in-the-management-of-shoulder-instability-23-2048.jpg)
![• The Instability severity index score[ ISIS] < 6pts
meant an acceptably rate of 10% instability
recurrence & potentially good candidates for
bankart procedure.
• Phandnis et al study with 141 pts, found a 7-%
risk of failure of arthroscopic ant. Stabilization
if ISIS >4 vs 4% risk if score < 4](https://image.slidesharecdn.com/currentconceptsinthemanagementofshoulderinstability-180922111952/75/Current-concepts-in-the-management-of-shoulder-instability-24-2048.jpg)


This document discusses the current concepts in the management of shoulder instability. It covers the causes, classifications, investigations, and treatment options for shoulder instability. For treatment, it emphasizes the importance of a systematic approach that considers the patient's age, activity level, and nature of the soft tissue and bony injuries. Non-operative treatments include physiotherapy, while operative options depend on the specific injuries and may include arthroscopic bankart repair, open latarjet procedure, remplissage, or capsular shift procedures. The goal of treatment and rehabilitation is to return the patient to their prior level of function and activity.
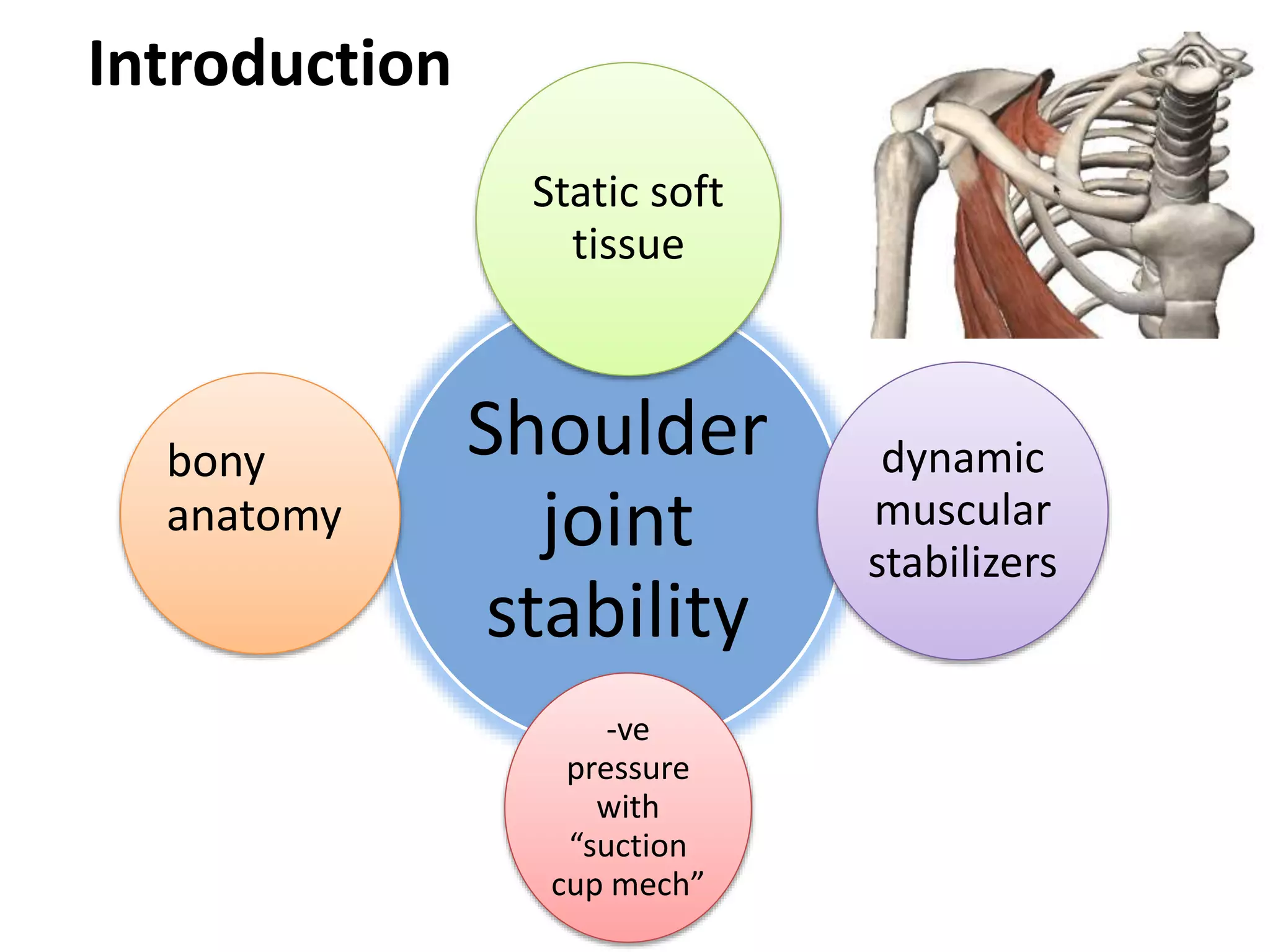
Discusses shoulder instability (SI) and its management, highlighting joint stability, causes, and increasing incidence in young, active individuals.
Examines the pain and dysfunction of shoulder instability in athletes, with an unknown incidence rate in India.
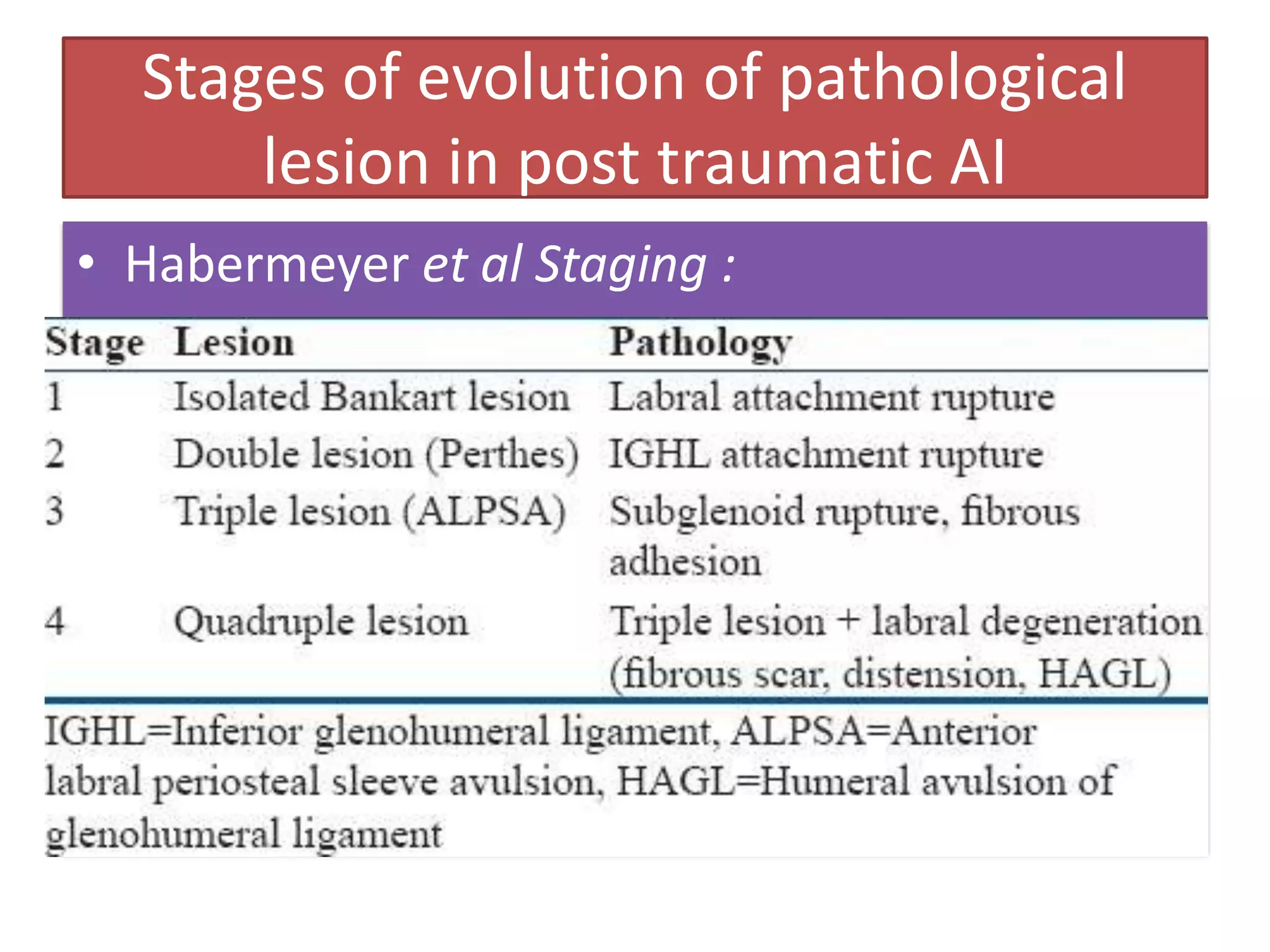
Outlines the stages of pathological lesions in post-traumatic anterior instability based on Habermeyer et al.
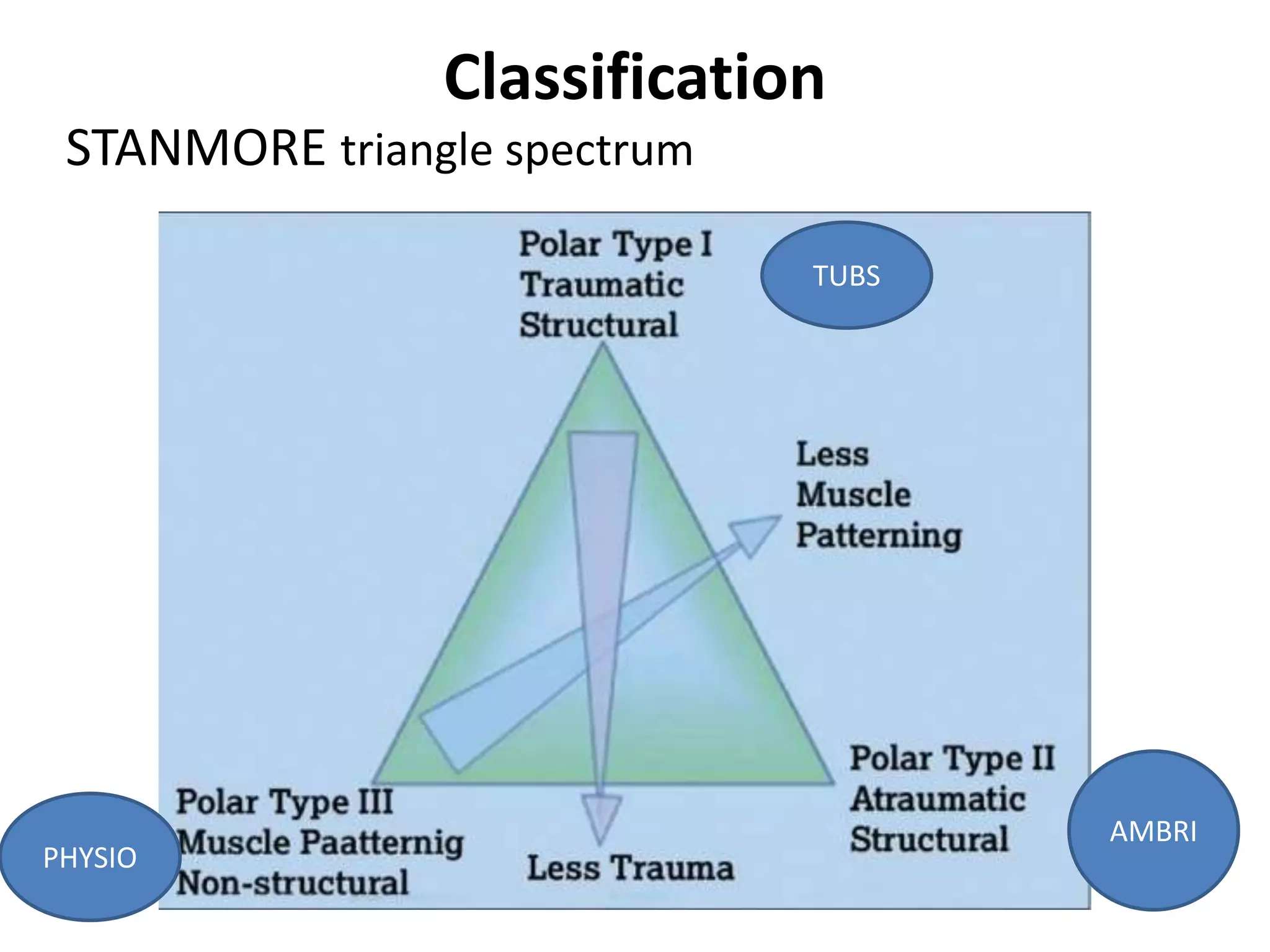
Introduces the classification of shoulder instability using STANMORE triangle spectrum, TUBS, AMBRI, and PHYSIO.
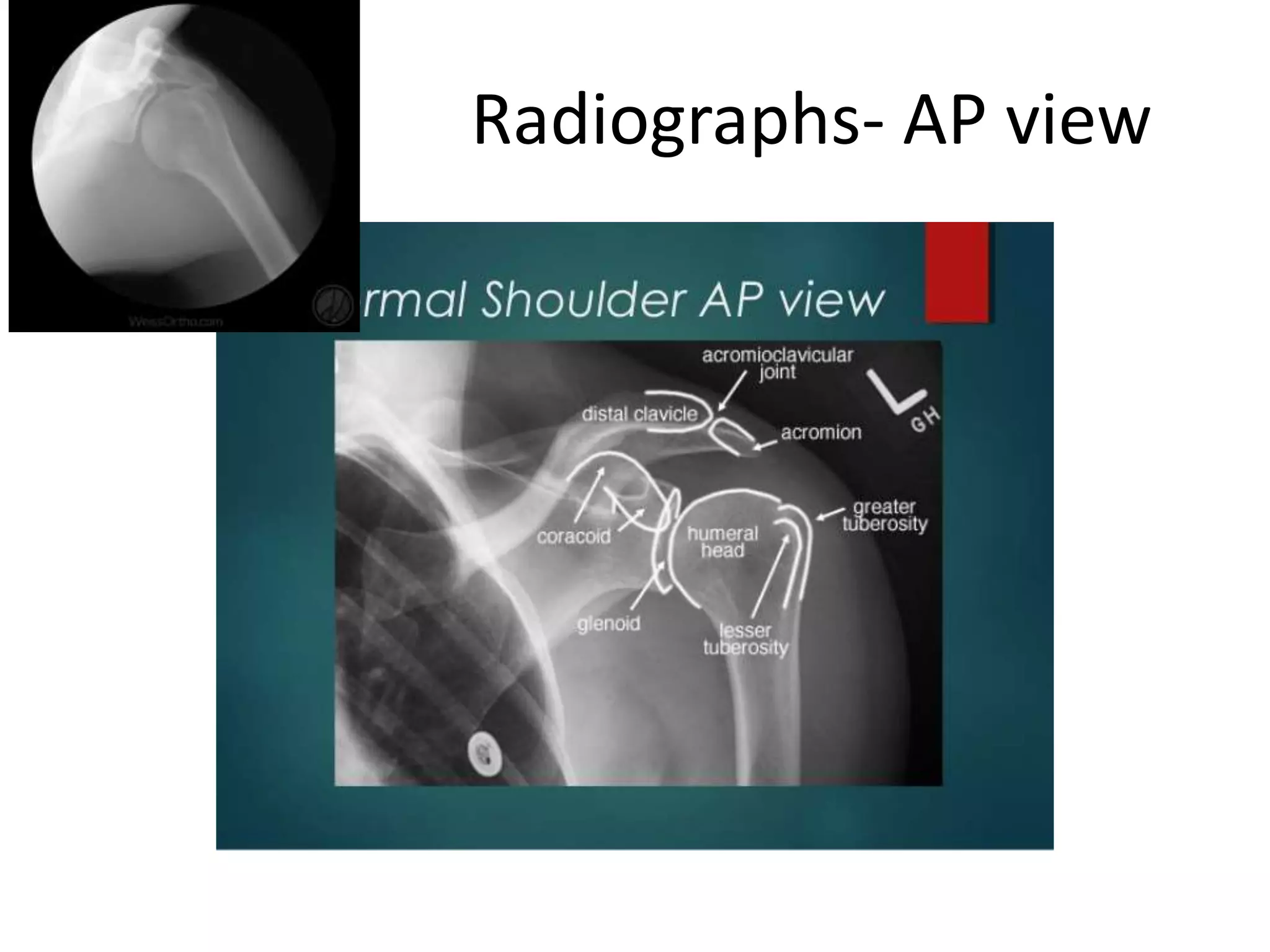
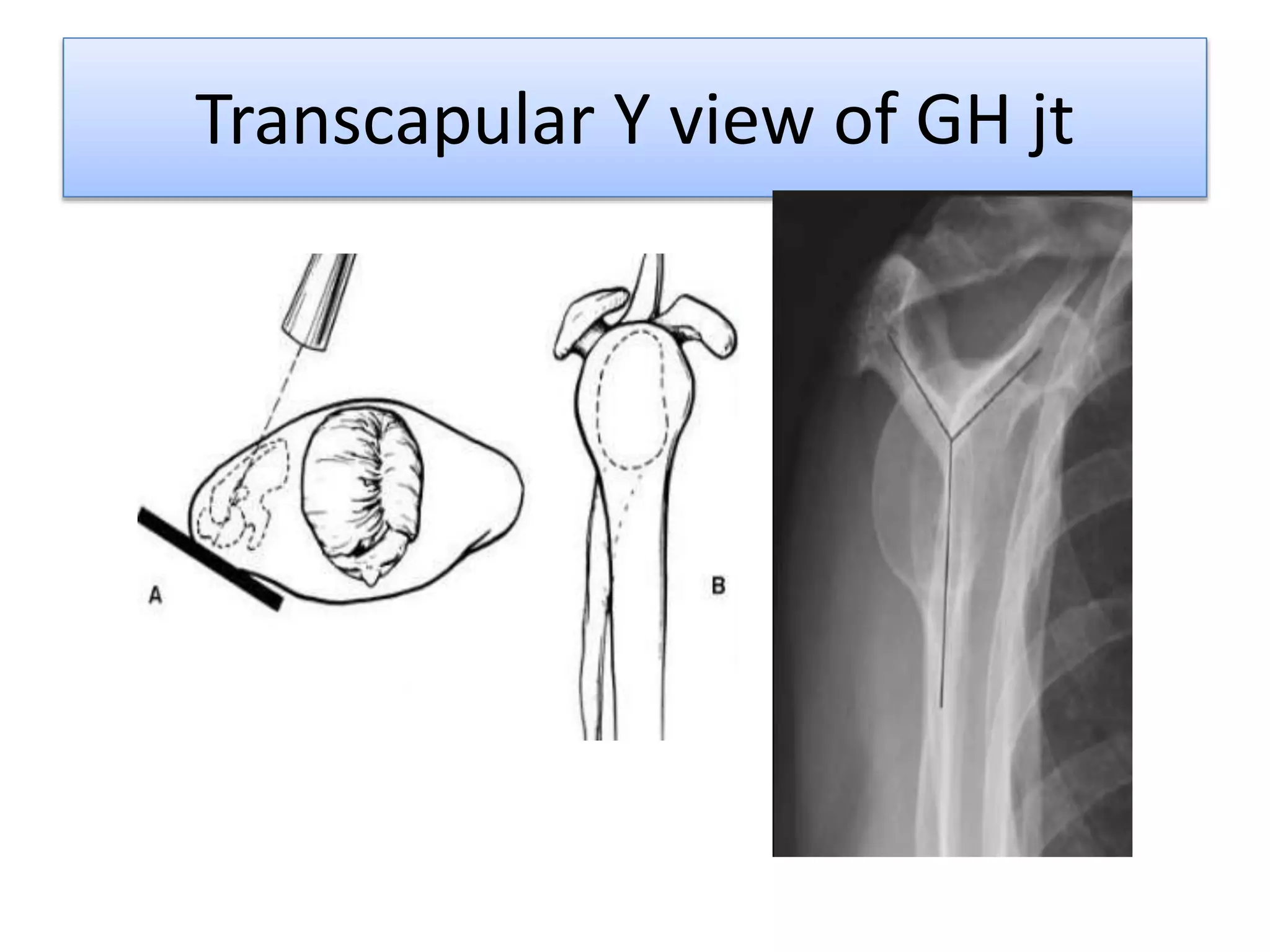
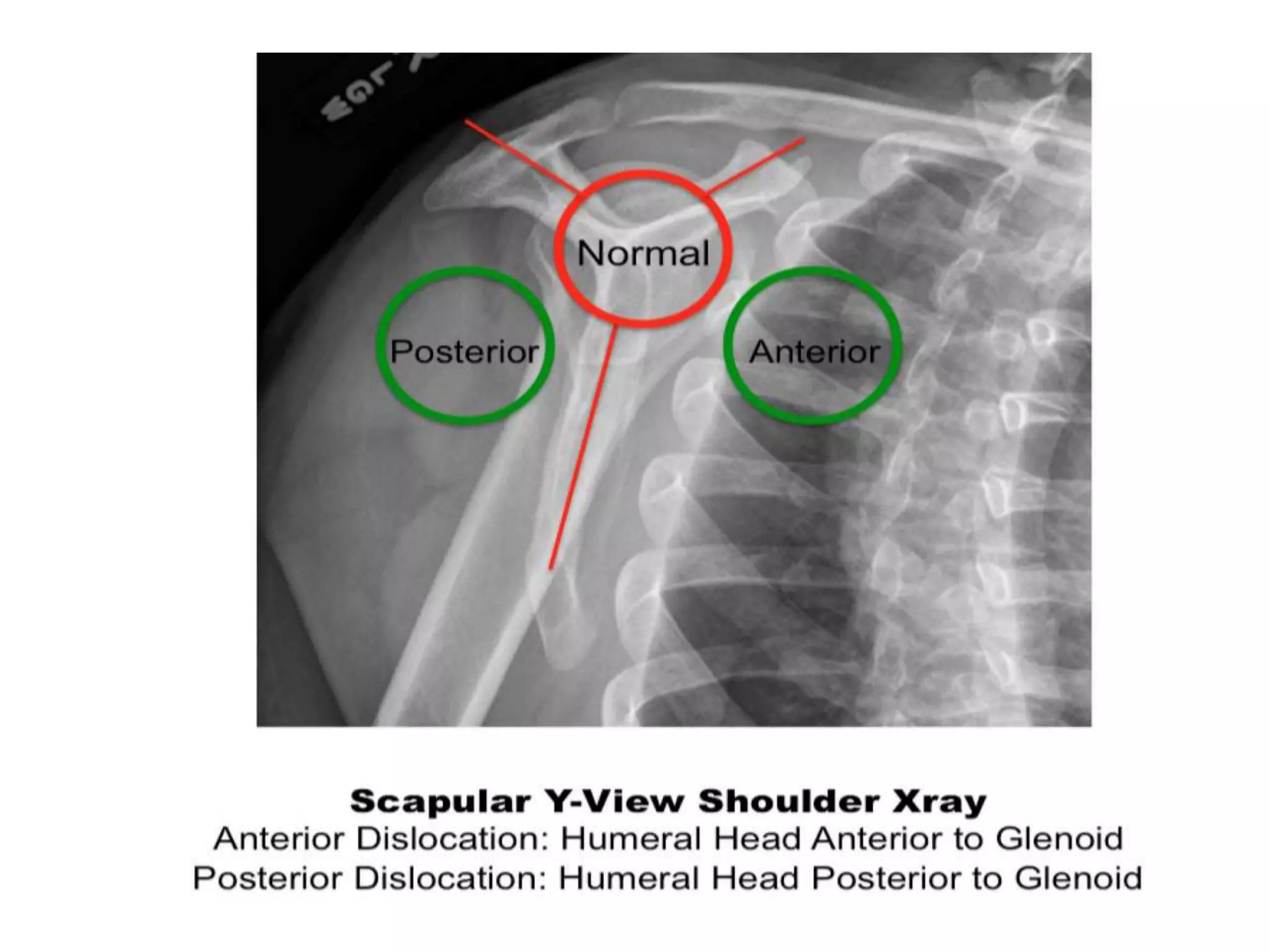
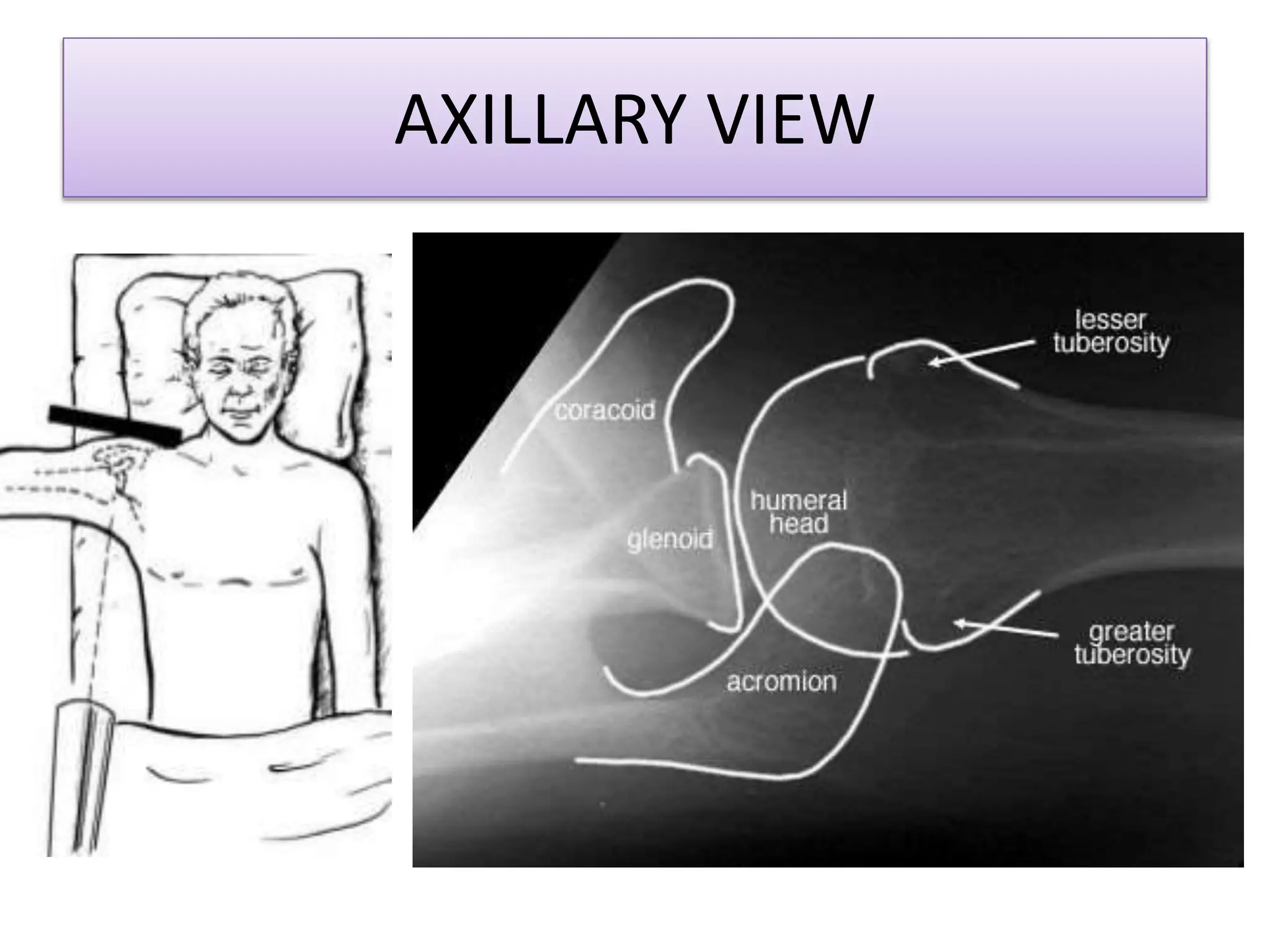
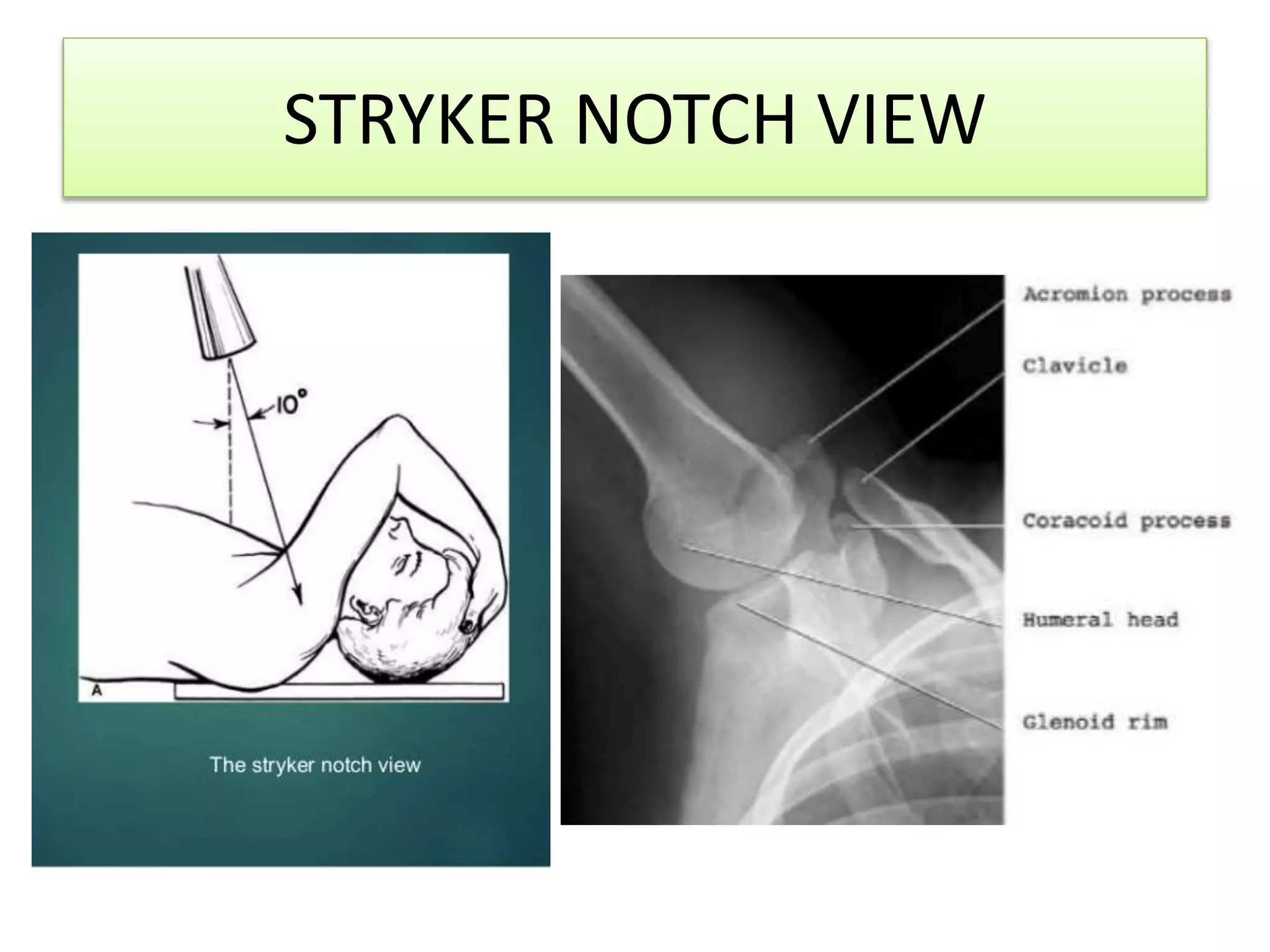
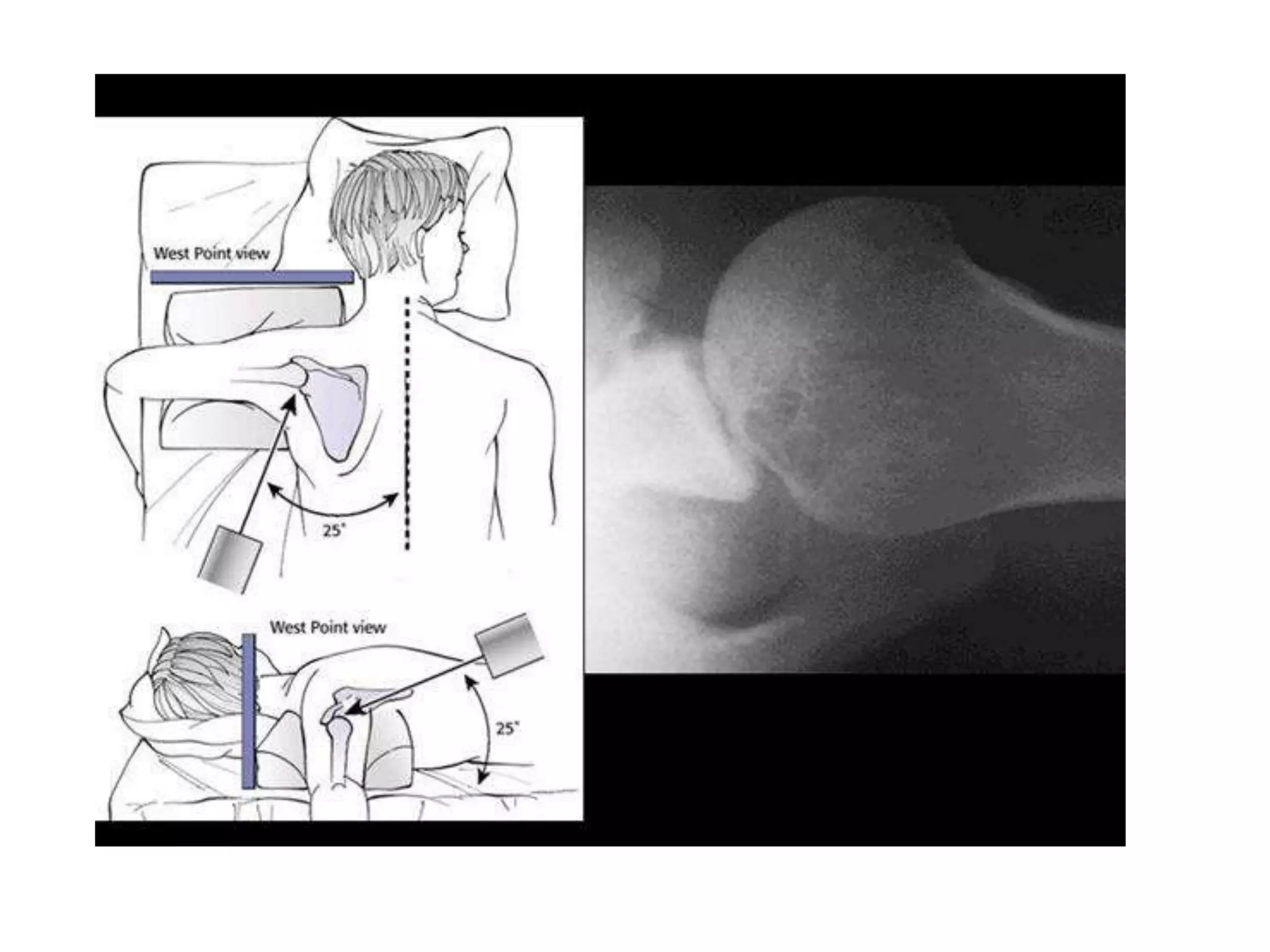
Details various imaging views—AP, Transcapular Y, Axillary, and Stryker Notch—to diagnose shoulder conditions.
Emphasizes the use of CT and MRI arthrograms for soft tissue and bony pathology assessment to guide surgical approaches.
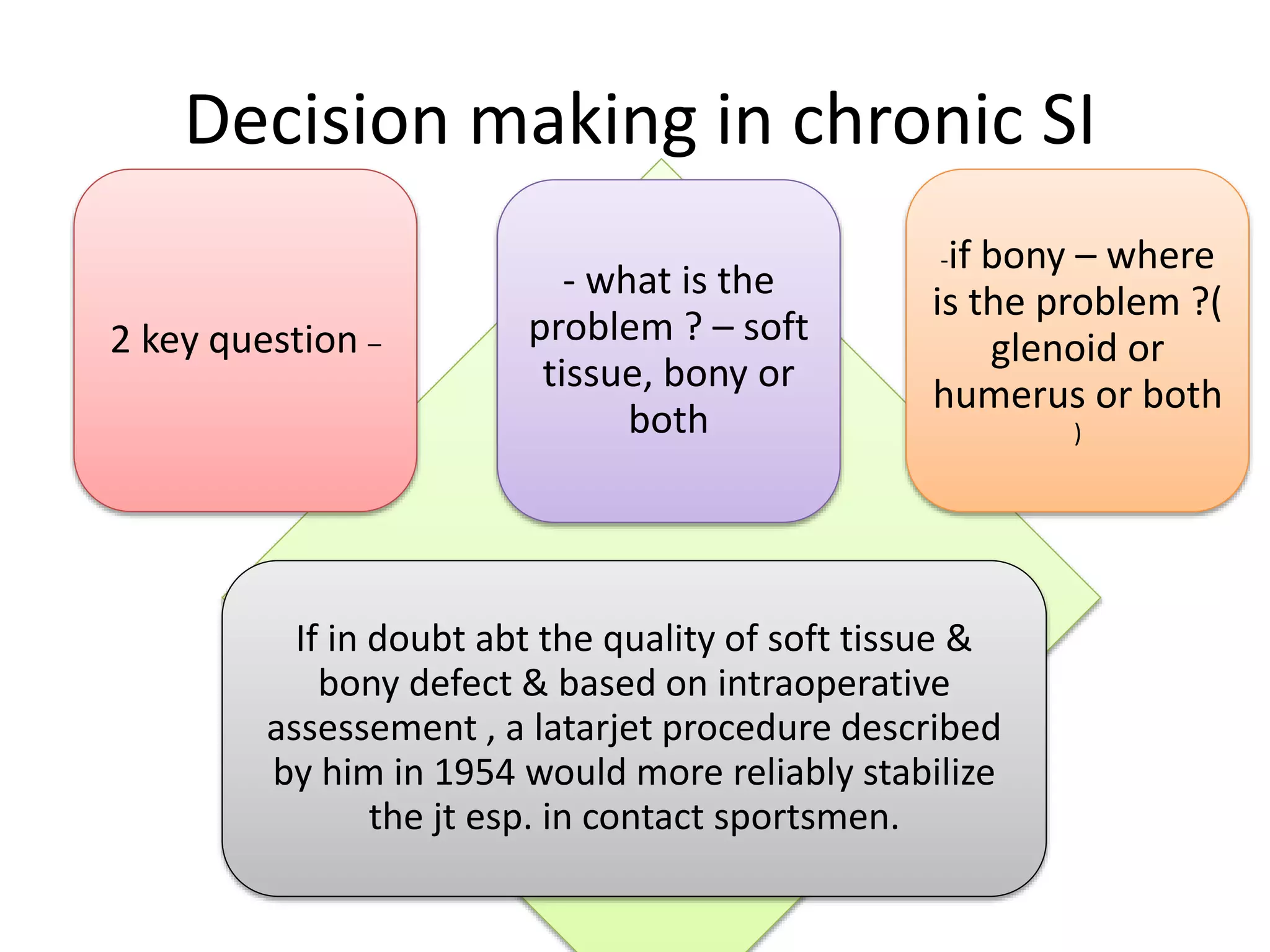
Explains non-operative and operative management for anterior instability, highlighting factors influencing surgical decisions.
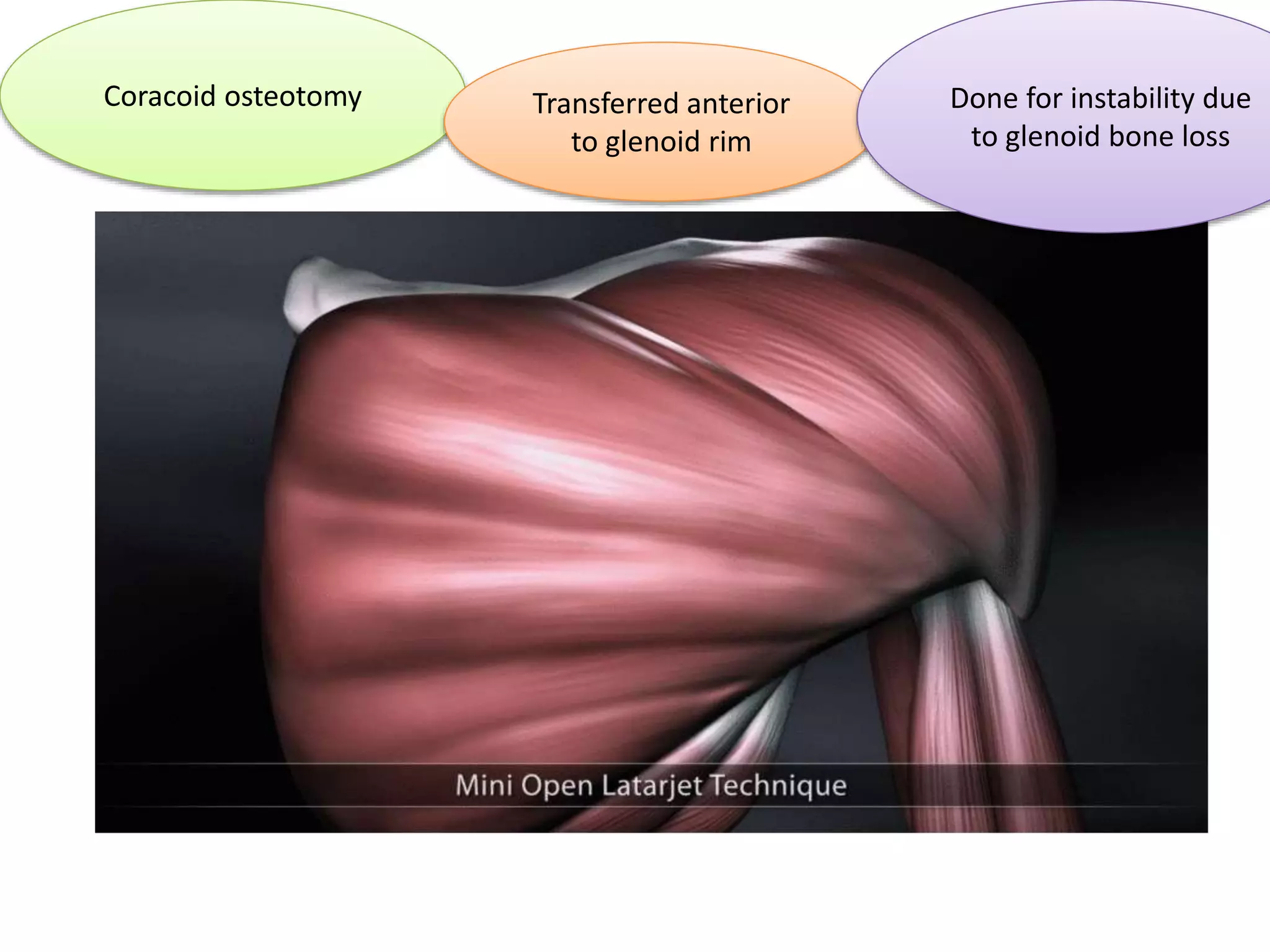
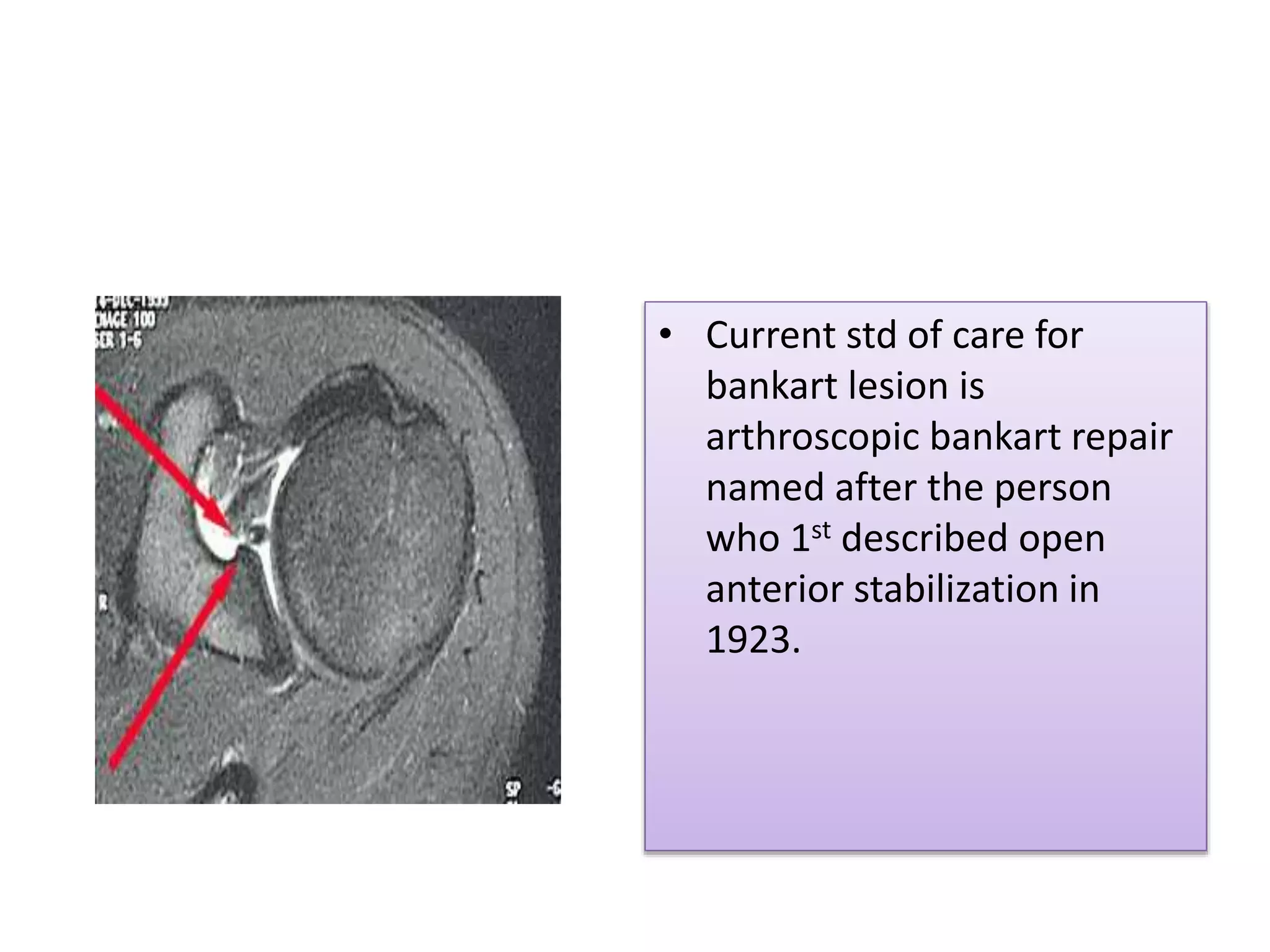
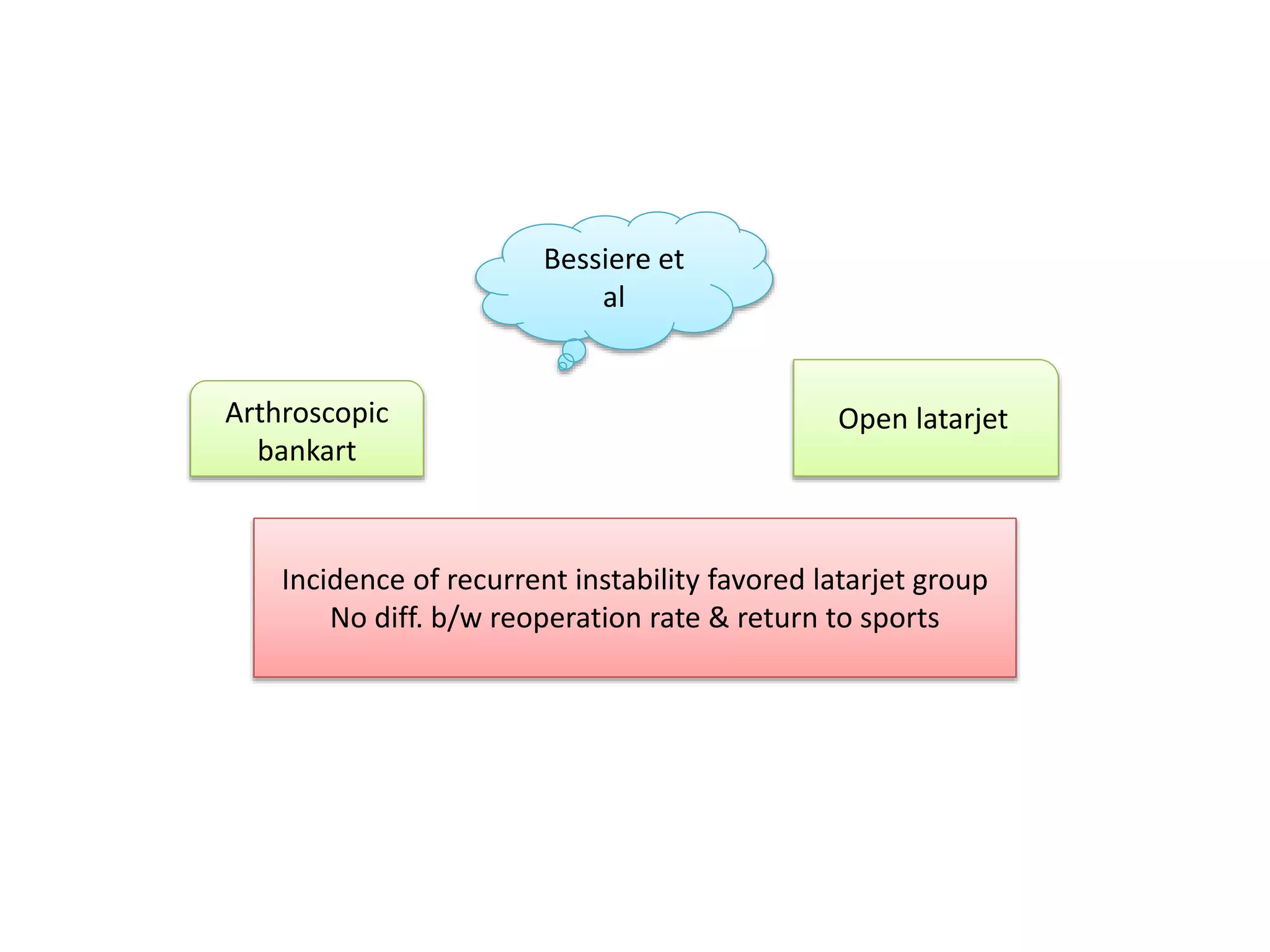
Describes the Latarjet procedure for significant glenoid defects and the standard of care for Bankart lesions.
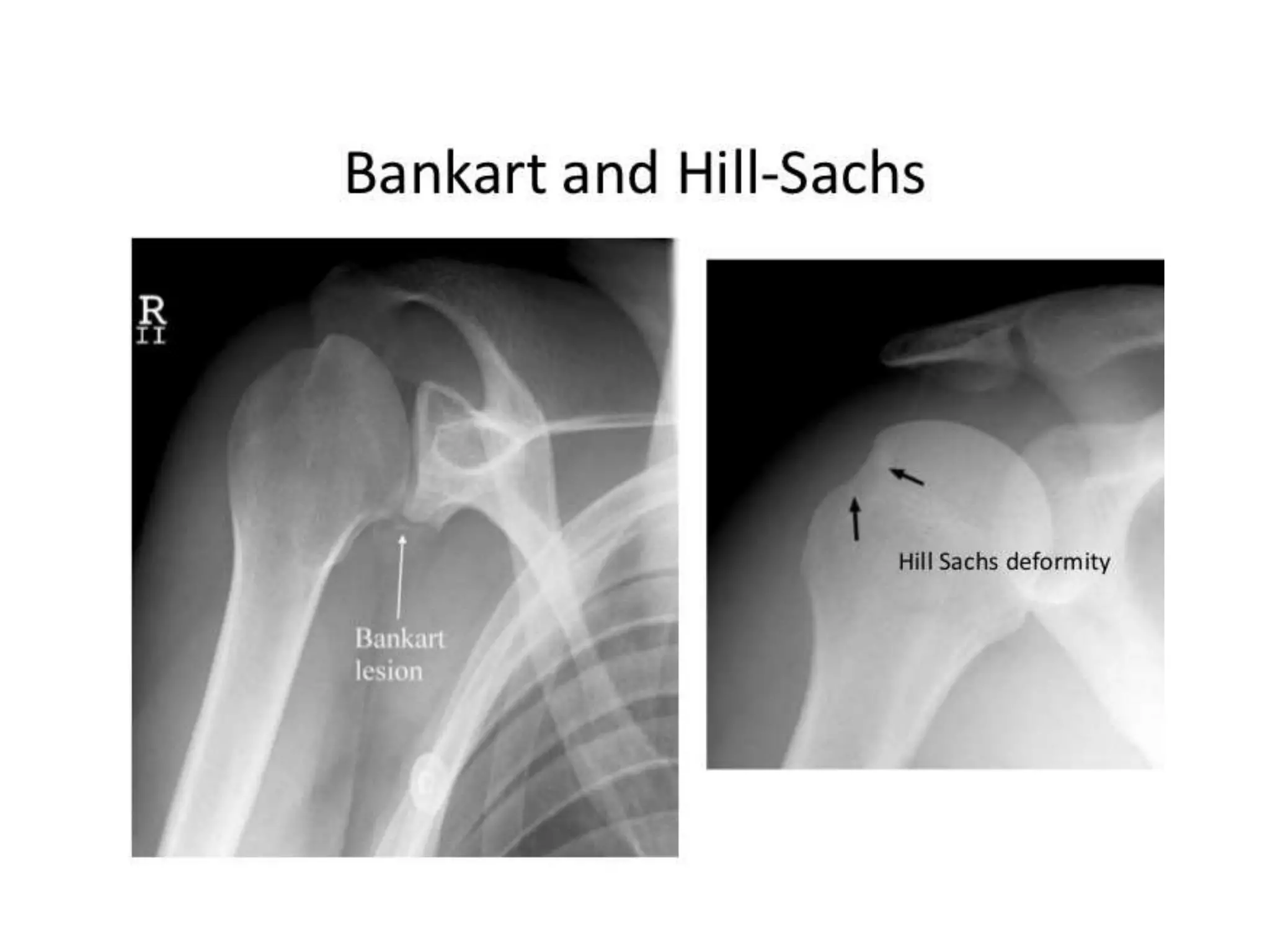
Highlights the importance of considering both Bankart and Hill-Sachs lesions in instability and introduces glenoid tracking concepts.
Discusses the arthroscopic reimplissage procedure for large Hill-Sachs lesions in conjunction with anterior repairs.
Presents ISIS scoring system to evaluate recurrence risk post-surgery, linking it to arthroscopic stabilization outcomes.
Outlines treatment options for multidirectional and posterior instability, with emphasis on arthroscopic techniques.
Focuses on rehabilitation strategies post-surgery aiming for a return to pre-injury functional status, particularly in athletes.
Concludes with comprehensive assessment and management strategies for shoulder instability, including the importance of investigations.
Thanks the audience and concludes the presentation.























































































