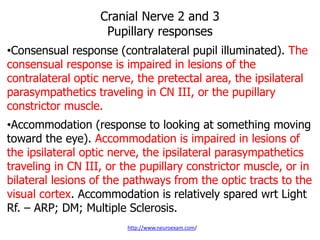
Downloaded 172 times

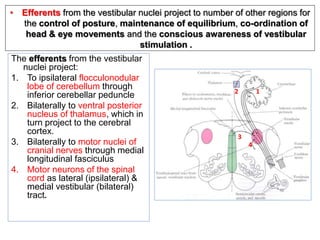
![PRELIMINARY
• Adequate Lighting/Exposure[Screen if
required]
• Comfort Patient
• Hand Wash/Rub; All equipment ready
• Explain testing procedure before
• Consent
• Be Gentle](https://image.slidesharecdn.com/cranialnerves-191225130034/85/Cranial-nerves-2-320.jpg)

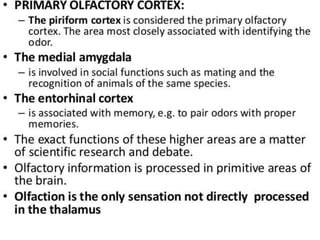


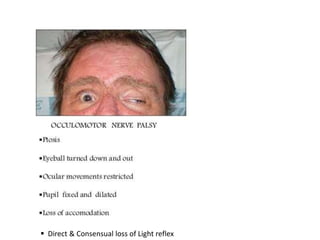













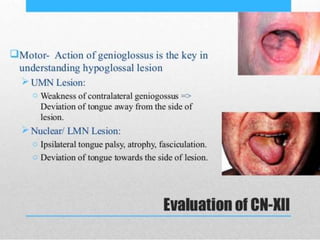
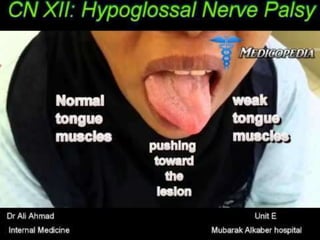
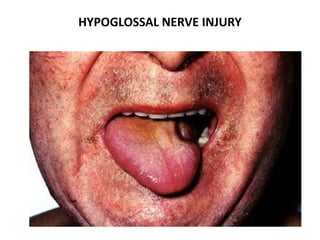
![CRANIAL NERVE XII
[LAST:”THANK GOD”]](https://image.slidesharecdn.com/cranialnerves-191225130034/85/Cranial-nerves-210-320.jpg)
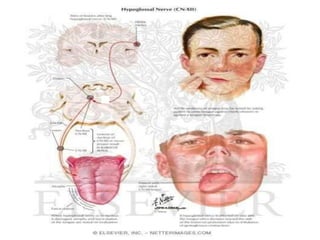
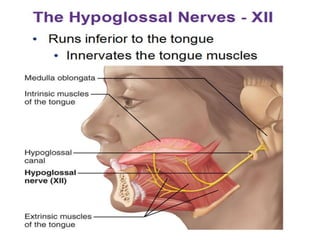
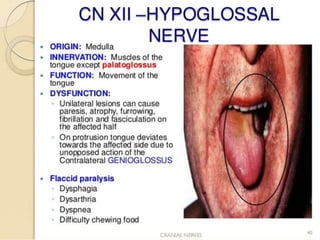
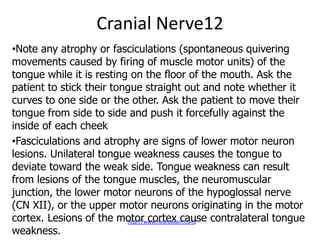
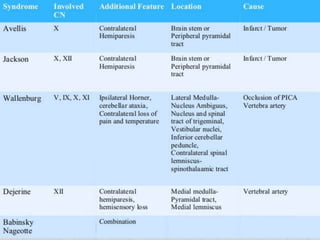
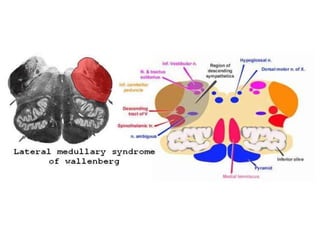
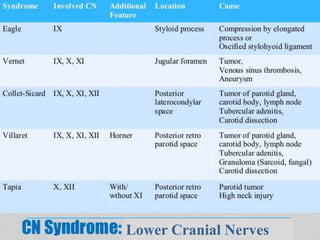
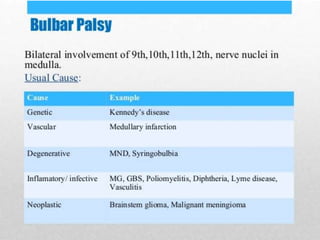
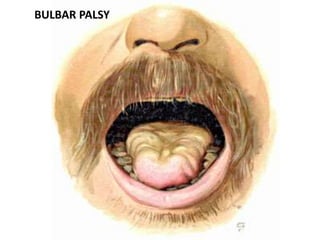
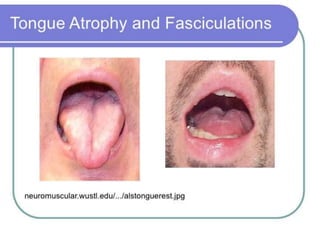

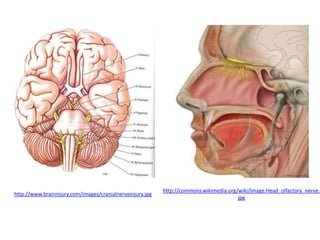
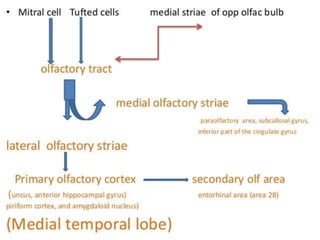
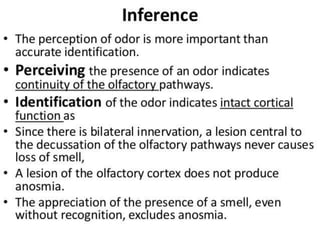
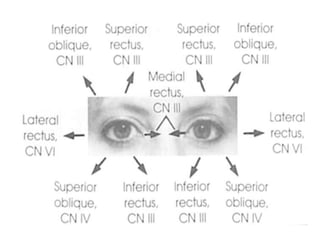
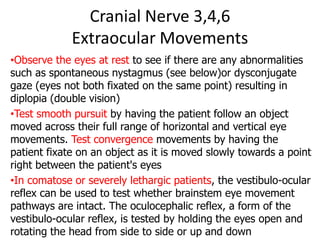
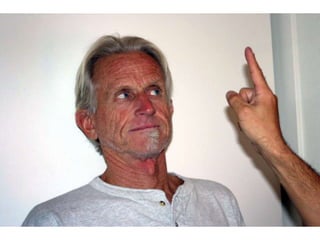
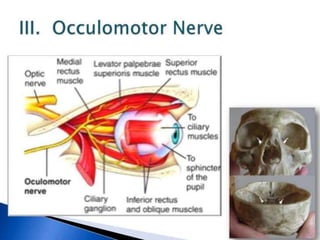
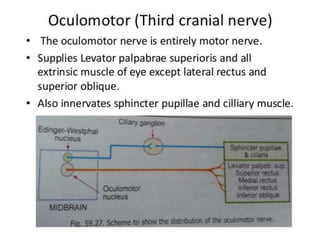
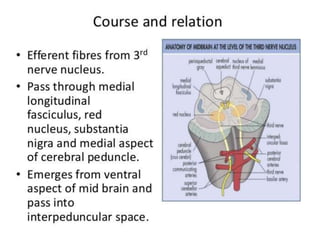
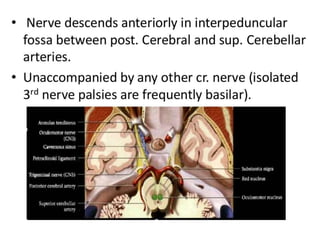
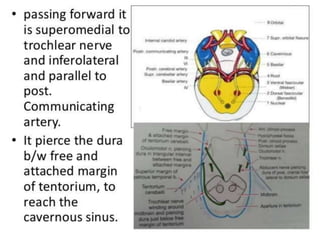
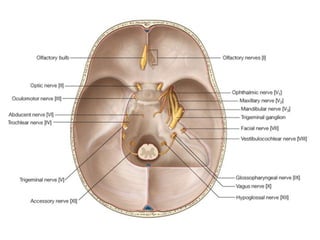
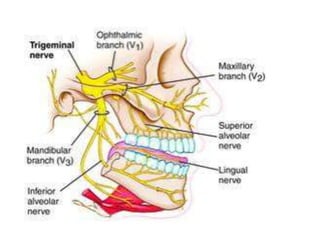
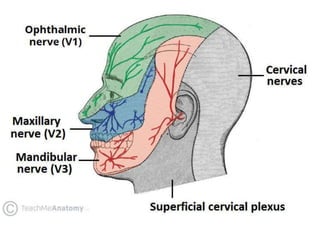
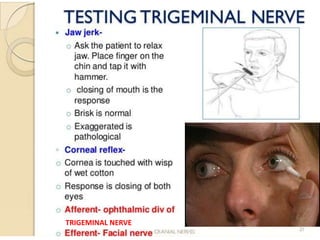
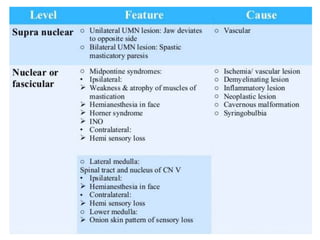
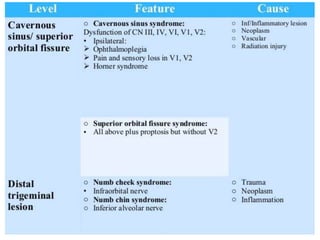
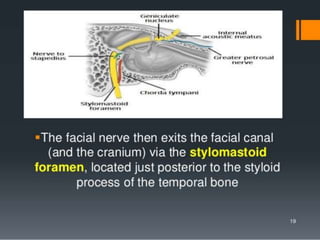
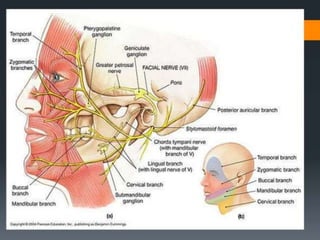
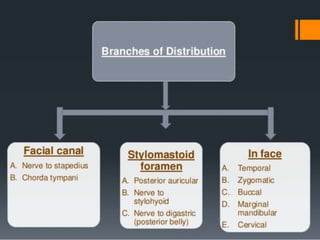
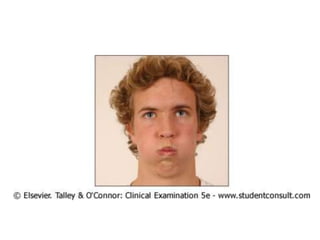
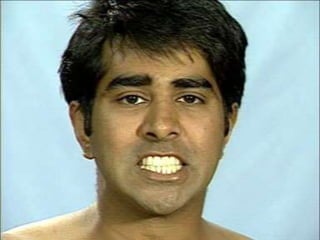
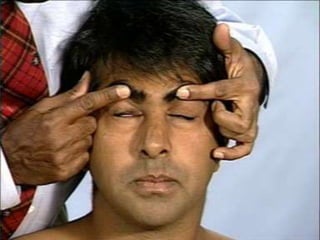
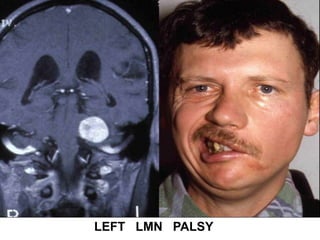
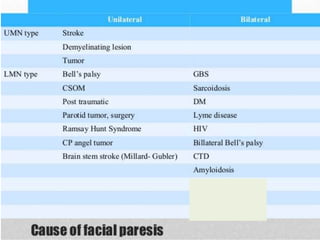
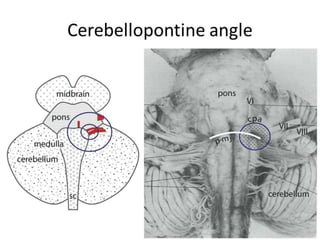
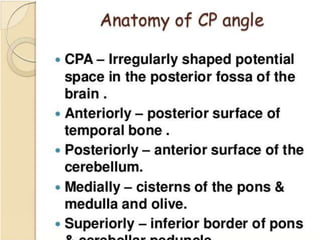
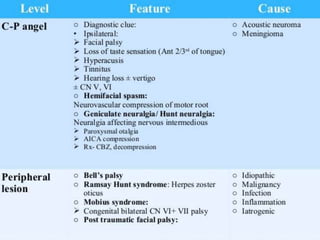
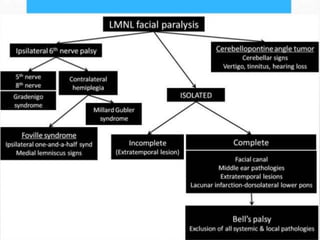
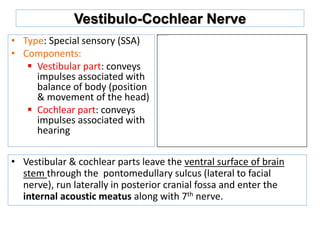
This document provides information about examining the 12 cranial nerves. It discusses approaches to testing each nerve including optimal positioning of the patient, specific maneuvers to assess nerve function, and potential causes of abnormalities. For each nerve, it describes the anatomical course and key structures innervated. The summary focuses on testing methodology: Cranial nerve examination involves positioning and comforting the patient, then testing individual nerves using specialized maneuvers like visual acuity tests, eye movement assessments, facial expression checks, and sensory evaluations to identify potential lesions. Proper lighting and explanation of procedures is important. Each nerve is analyzed for motor, sensory and reflex functions to localize neurological disorders.























































































