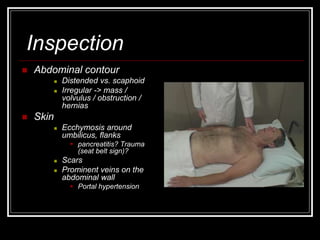
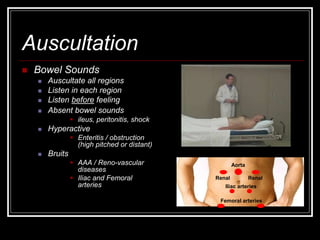
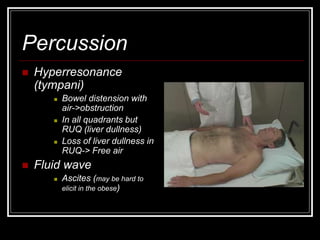
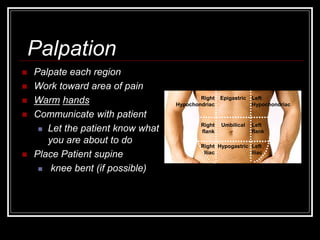
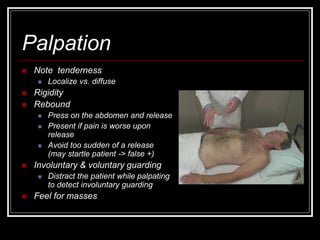
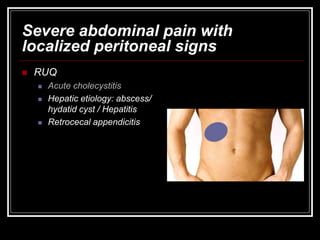
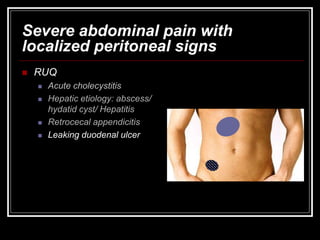
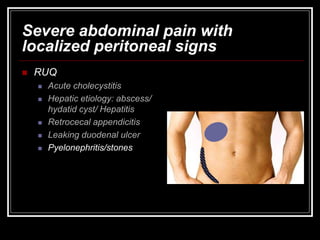
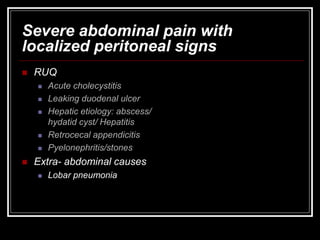
The document provides information on performing an abdominal exam, including objectives, techniques, findings, and differential diagnoses. It discusses examining the abdominal wall, vital signs, inspection, auscultation, percussion, and palpation. Specific findings that suggest conditions like appendicitis, peritonitis, or hemorrhage are outlined. Groupings of symptoms are presented with possible differential diagnoses.

























































![PRINCIPLES OF PHARMOCODYNAMICS 2 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/principlesofpharmocodynamics2autosaved-230607181037-758ddb07-thumbnail.jpg?width=640&height=640&fit=bounds)
































