Downloaded 187 times

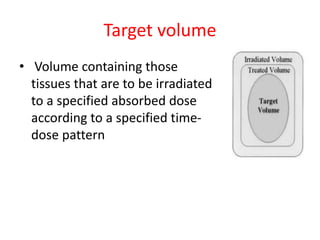
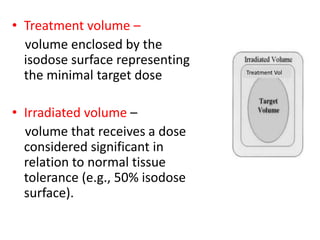
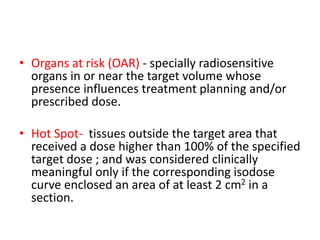
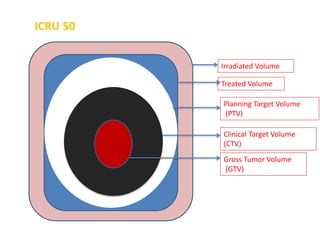
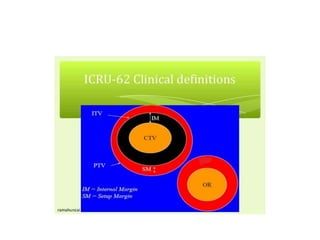
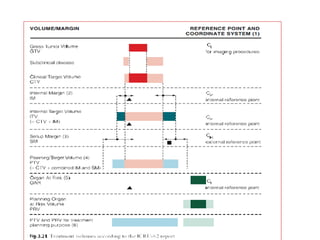
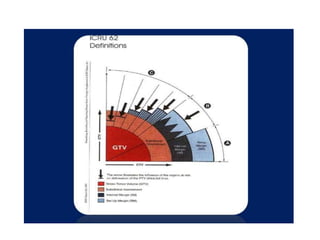

The document summarizes key ICRU reports related to external beam radiotherapy, including ICRU Reports 29, 50, and 62. Report 29 established definitions like target volume, treatment volume, and organs at risk. Report 50 refined definitions and introduced clinical target volume, planning target volume, and treated volume. Report 62 further refined margins and introduced internal margin and setup margin. It also defined planning organ at risk volume and conformity index. The reports provide recommendations for dose reporting including minimum, maximum, and reference doses.

![Arc therapy [autosaved] [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/arctherapyautosavedautosaved-150423125828-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)


































































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)











