Downloaded 350 times
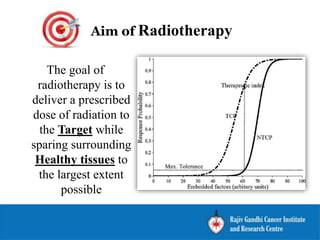
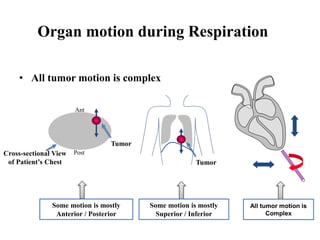
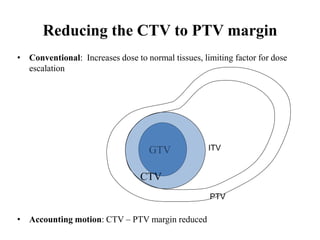
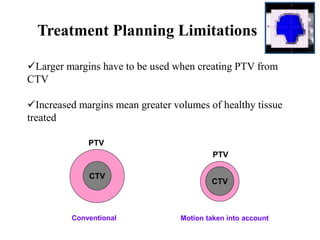
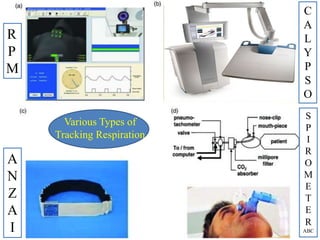
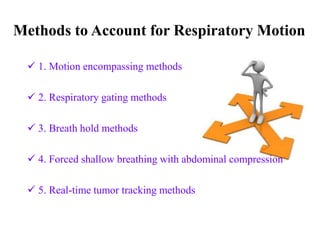

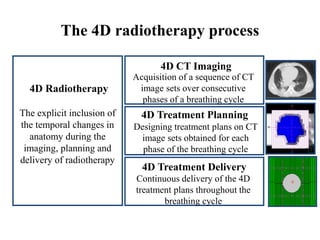
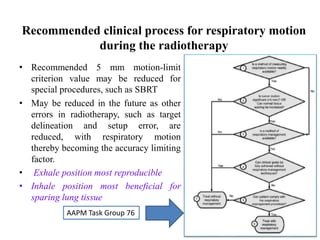


The document outlines the principles and challenges of managing respiratory motion in radiotherapy, emphasizing the importance of accurately targeting tumors while minimizing exposure to healthy tissues. It discusses various strategies for tumor motion tracking and treatment planning, including motion encompassing methods, respiratory gating, and real-time tracking technologies. The evolving nature of Image Guided Radiation Therapy (IGRT) is highlighted as a promising solution for enhancing treatment precision and effectiveness.




![Rrecent advances in linear accelerators [MR linac]](https://cdn.slidesharecdn.com/ss_thumbnails/icroproadvance2021-recentadvancesinlinearaccelerators-211201040416-thumbnail.jpg?width=640&height=640&fit=bounds)









![Arc therapy [autosaved] [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/arctherapyautosavedautosaved-150423125828-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)



















































