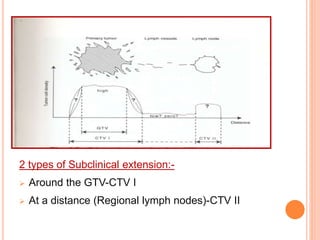
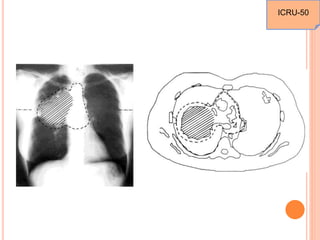
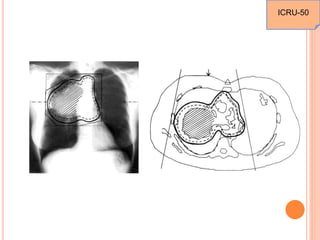
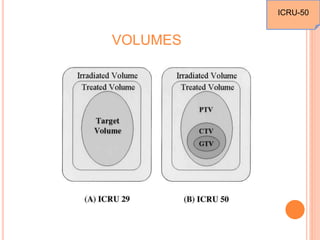
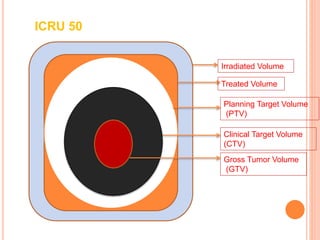
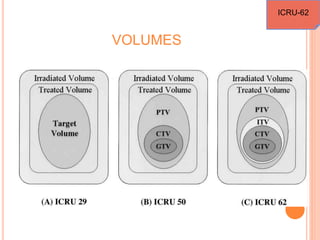
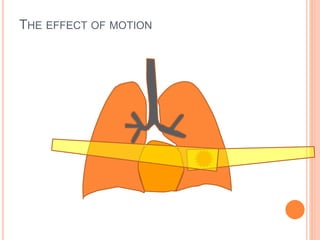
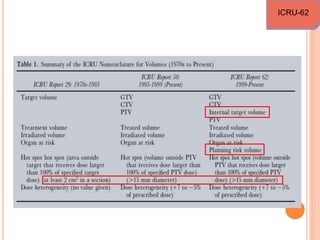
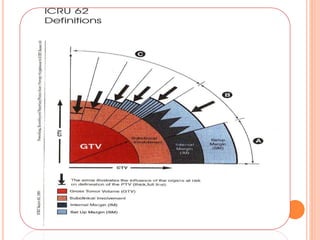
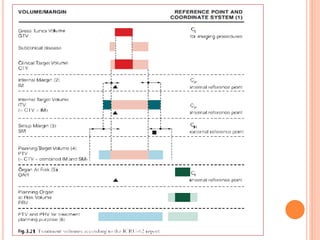
The document discusses recommendations from ICRU reports 50 and 62 regarding prescribing, recording, and reporting photon beam radiation therapy. ICRU Report 50 from 1993 establishes definitions for key volumes used in treatment planning like gross tumor volume, clinical target volume, planning target volume, treated volume, and irradiated volume. ICRU Report 62 from 1999 supplements Report 50 by providing more details on margins needed to account for anatomical variations and uncertainties. It also defines volumes like internal target volume, internal margin, and planning organ at risk volume. The reports aim to standardize terminology and parameters for comparing treatment outcomes across institutions.

















![Arc therapy [autosaved] [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/arctherapyautosavedautosaved-150423125828-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)




















































