Downloaded 465 times
![Cairo-Bishop Definition of Clinical
Tumor Lysis Syndrome
• 1. Renal failure (creatinine[*]: ≥1.5 ULN[†] [age >12 yr or
age adjusted])
• 2. Cardiac arrhythmia/sudden death[*]
• 3. Seizure[*]
*Not directly or probably attributable to a therapeutic agent (e.g., rise in creatinine after amphotericin
administration).
† Patients will be considered to have elevated creatinine if their serum creatinine is 1.5 times greater
than the institutional upper limit of normal (ULN) below age/gender defined ULN. If not specified
by an institution, age/sex ULN creatinine may be defined as: >1 <12 years, both male and female,
61.6 mol/L; ≥12 <16 years, both male and female, 88 μmol/L; ≥16 years, female, 105.6 μmol/L; ≥16
years, male, 114.4 μmol/L.
•](https://image.slidesharecdn.com/tumourlysissydrome-170706081350/85/Tumour-lysis-sydrome-8-320.jpg)
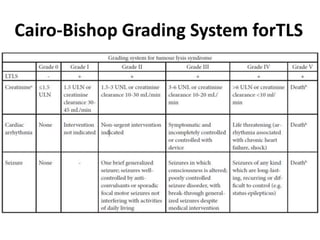
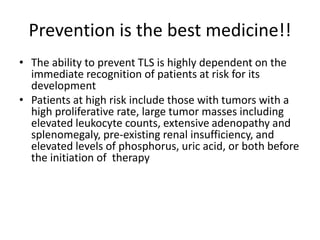
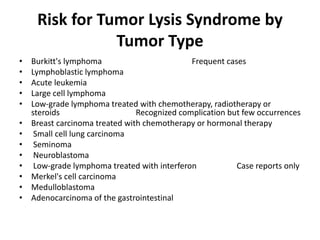
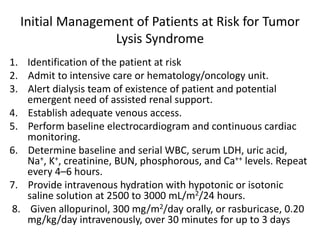
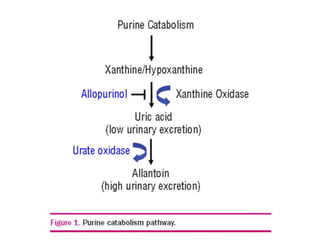
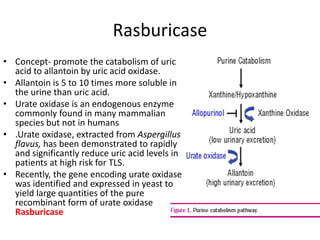

Tumor lysis syndrome (TLS) describes metabolic derangements that occur from rapid tumor breakdown associated with cytotoxic therapy. It is characterized by hyperuricemia, hyperkalemia, hyperphosphatemia, and hypocalcemia. TLS requires immediate intervention as it can overwhelm homeostatic mechanisms. It occurs primarily in hematologic malignancies with high proliferation rates that are sensitive to therapy. Prevention through hydration, hypouricemic agents, and monitoring of at risk patients is important to manage TLS.
















































































