Downloaded 522 times









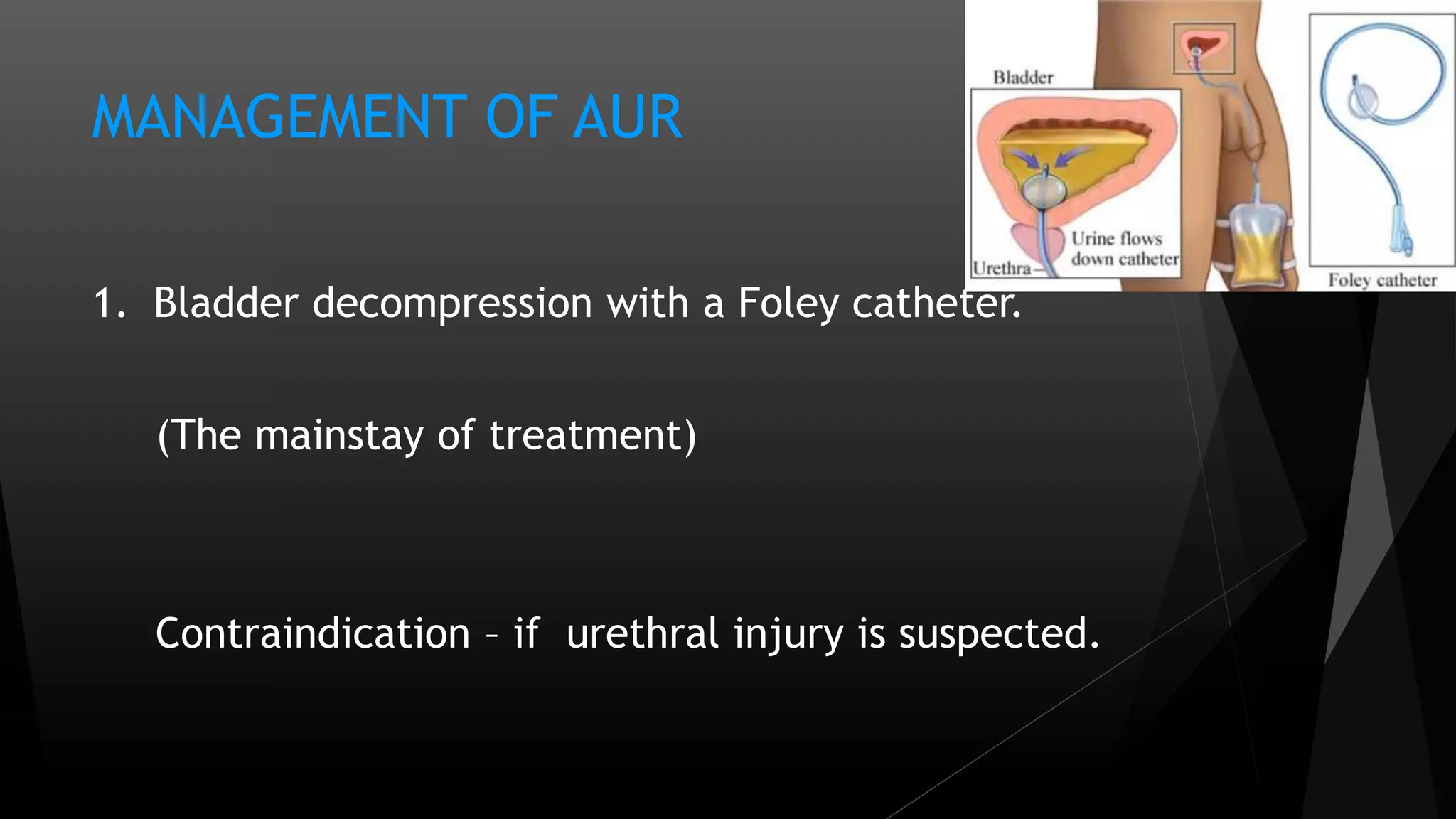







Acute urinary retention (AUR) is a urological emergency characterized by a sudden inability to void the bladder, primarily affecting men. Key risk factors include age over 70, prostate enlargement, and urinary flow issues, with common causes being benign prostatic hypertrophy and neurological impairments. Management involves bladder decompression through catheterization, with surgical options for underlying conditions and monitoring for complications.



































































