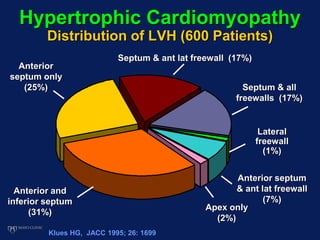
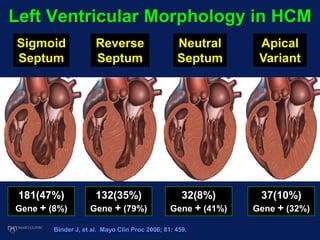
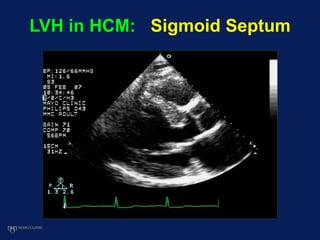
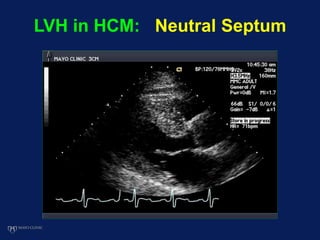
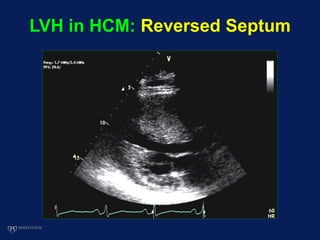
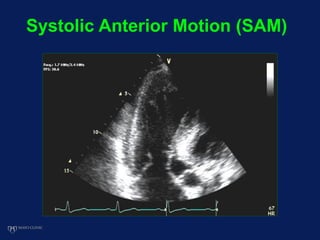
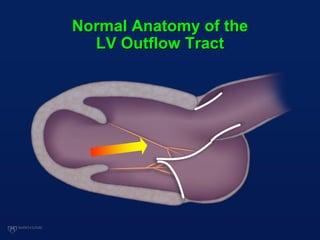
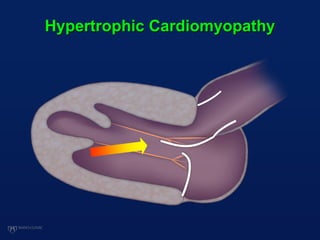
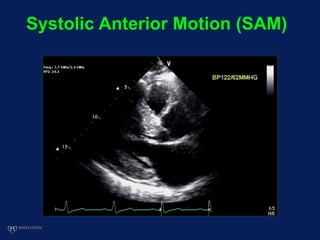
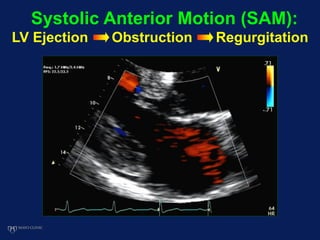
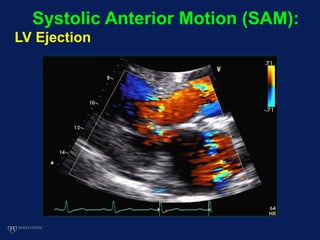
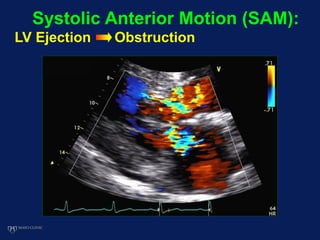
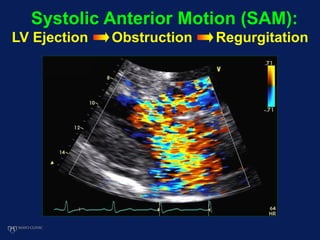
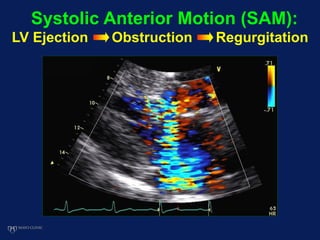
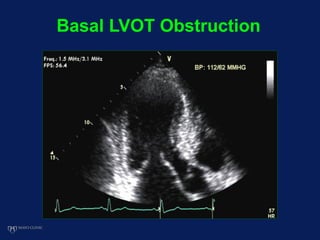
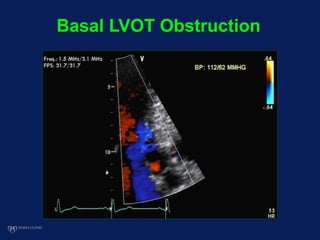
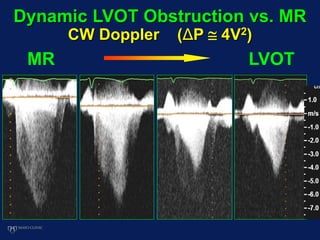
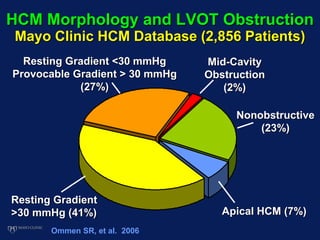
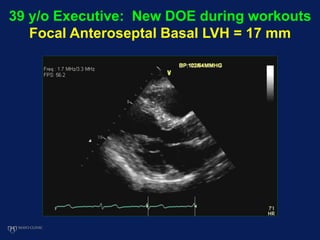
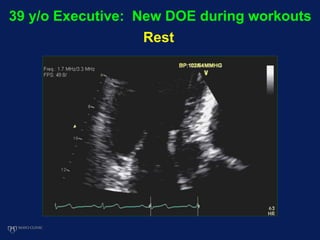
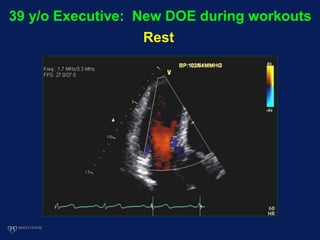
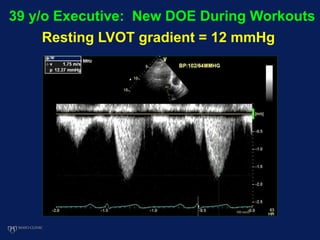
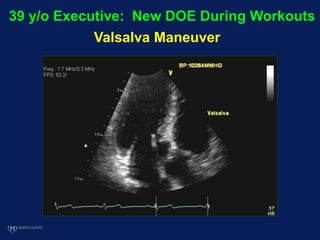
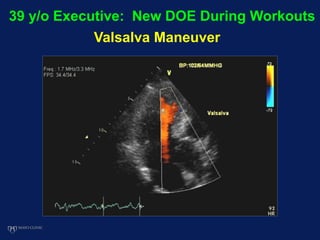
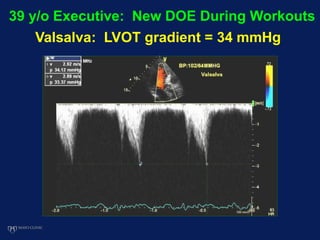
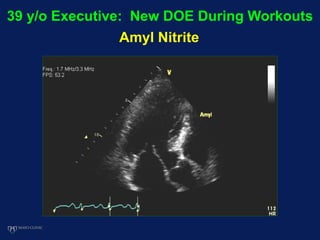
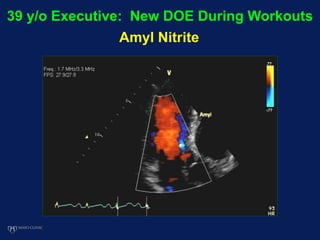
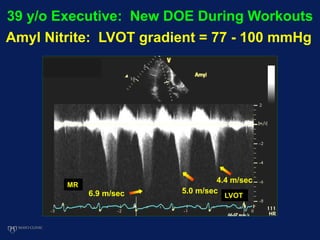
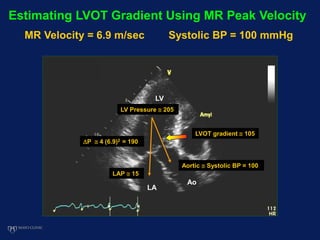
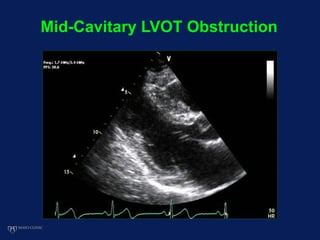
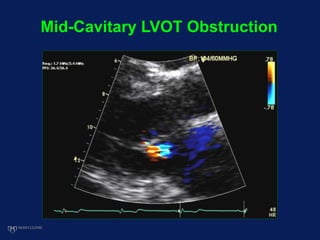
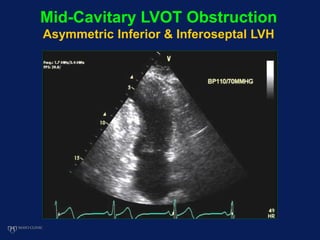
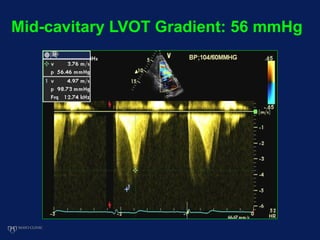
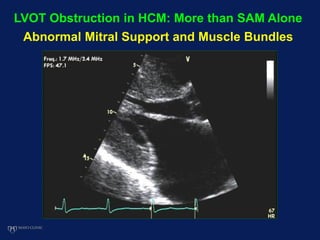
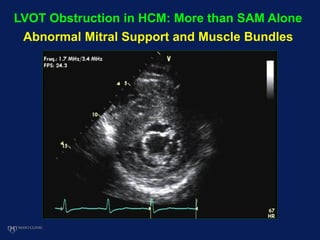
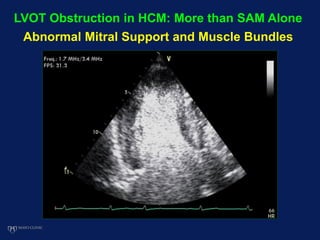
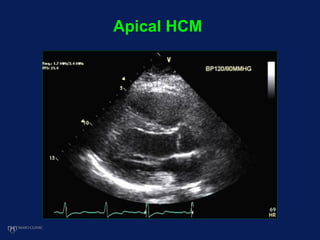
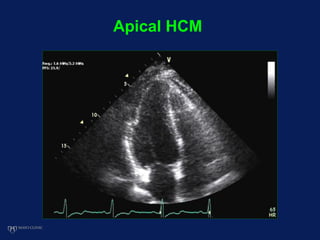
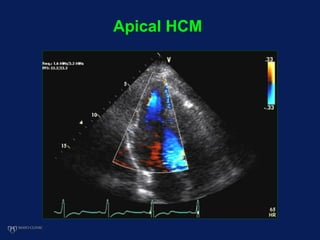
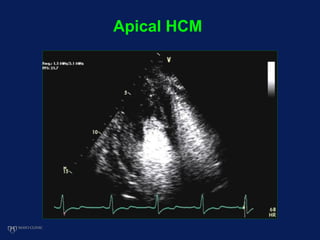
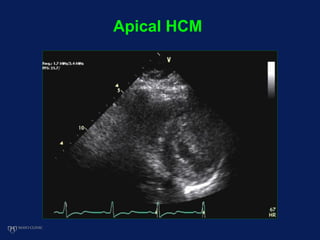
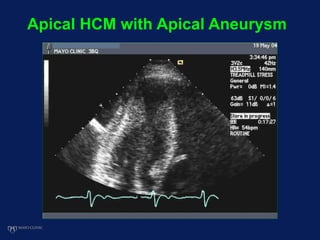
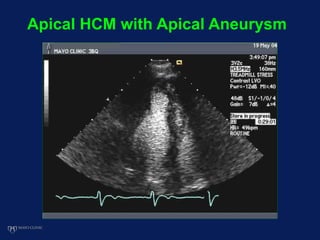
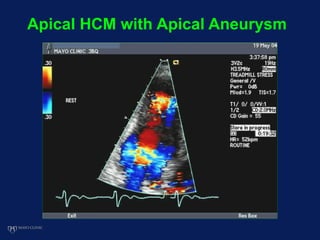
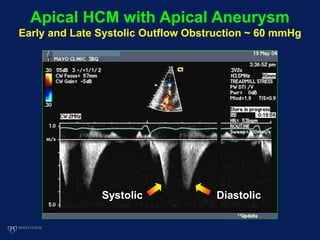
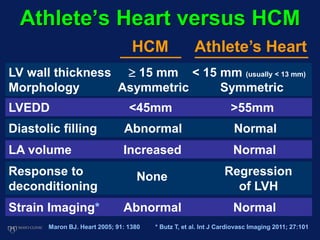
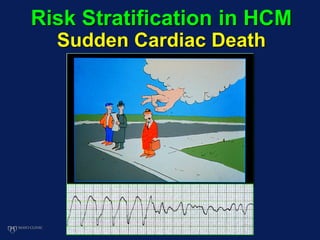
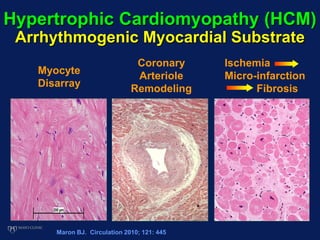
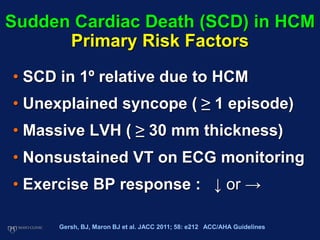
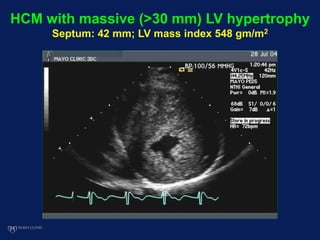
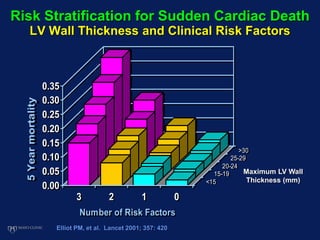
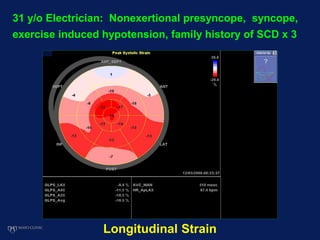
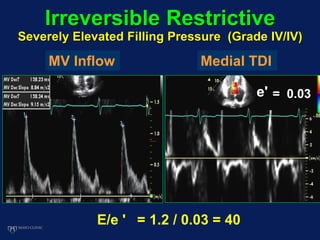
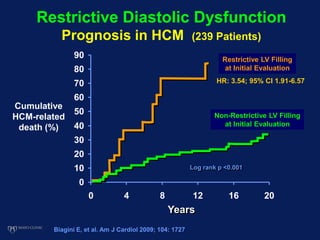
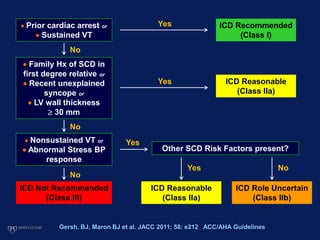
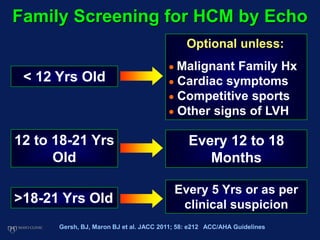
Echocardiography plays an essential role in diagnosing hypertrophic cardiomyopathy (HCM) by demonstrating left ventricular hypertrophy of 15mm or greater that is asymmetric and cannot be attributed to another cause. Echocardiography can also identify the characteristic patterns of hypertrophy such as sigmoid septum, reverse curvature of the septum, and apical hypertrophy. It is used to detect complications of HCM such as left ventricular outflow tract obstruction, mitral regurgitation, and apical aneurysms. Risk stratification for sudden cardiac death utilizes echocardiography to identify features such as massive hypertrophy, abnormal blood pressure response to exercise, and nonsustained ventricular tachycard

























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


