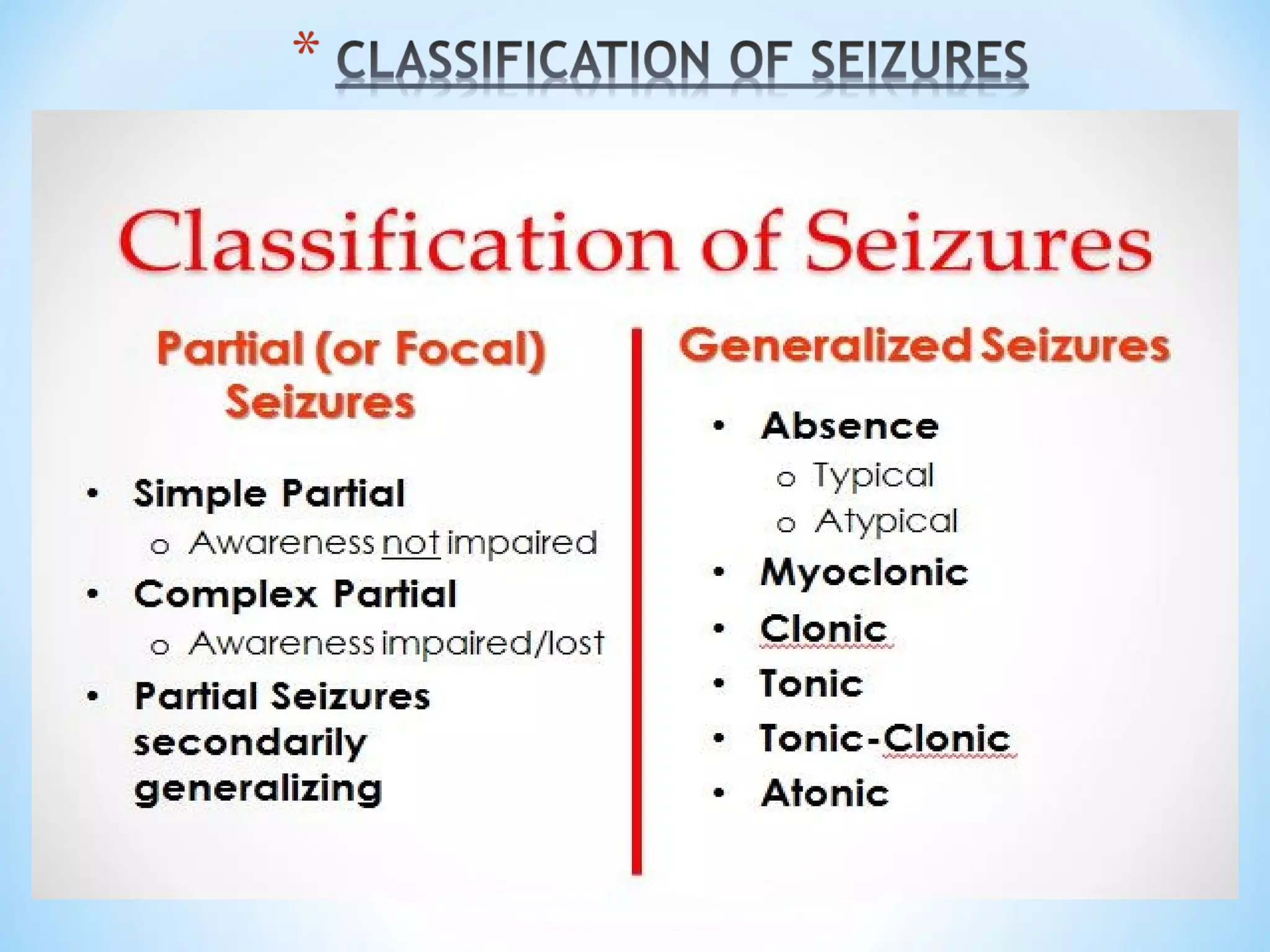
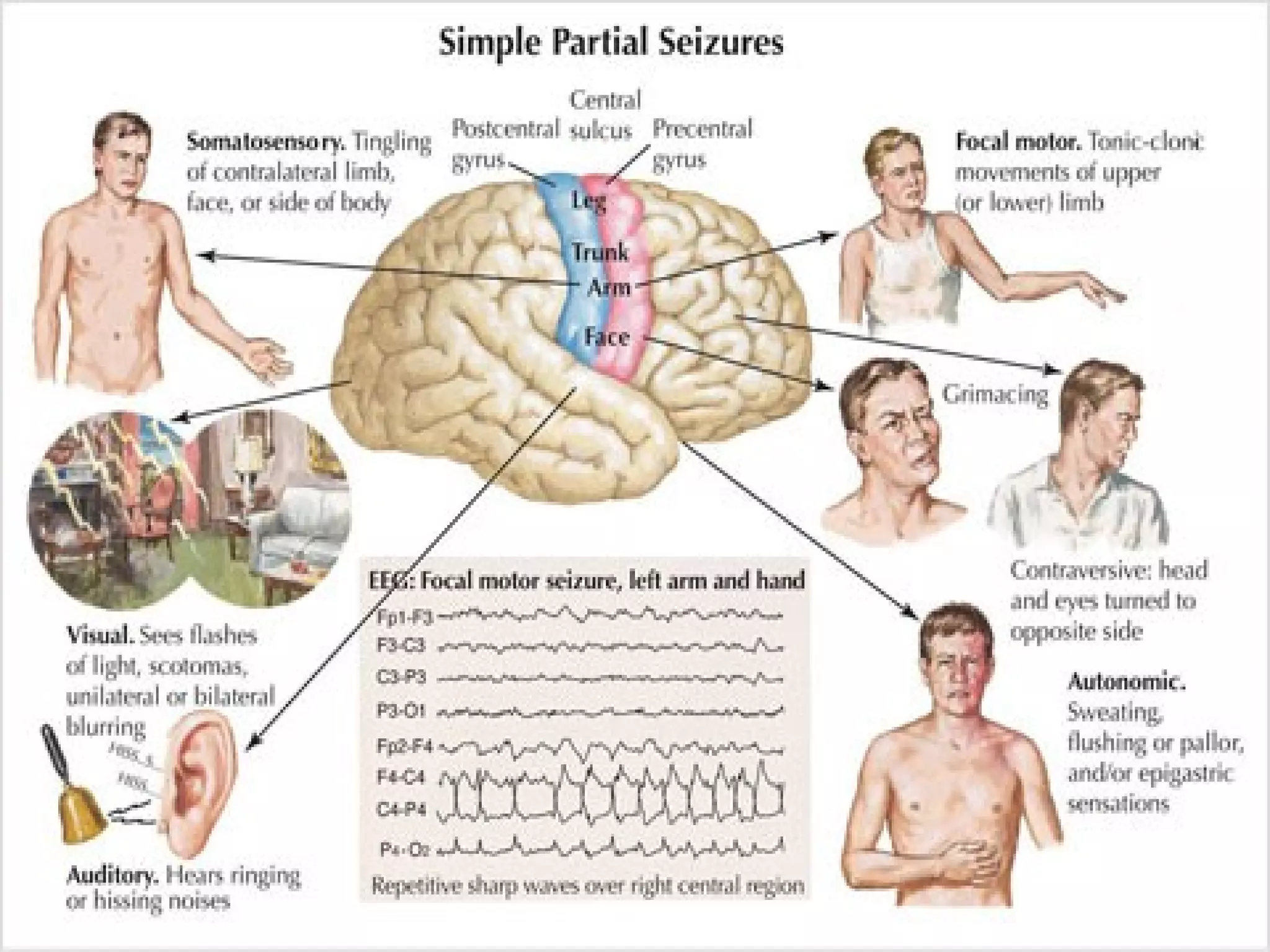
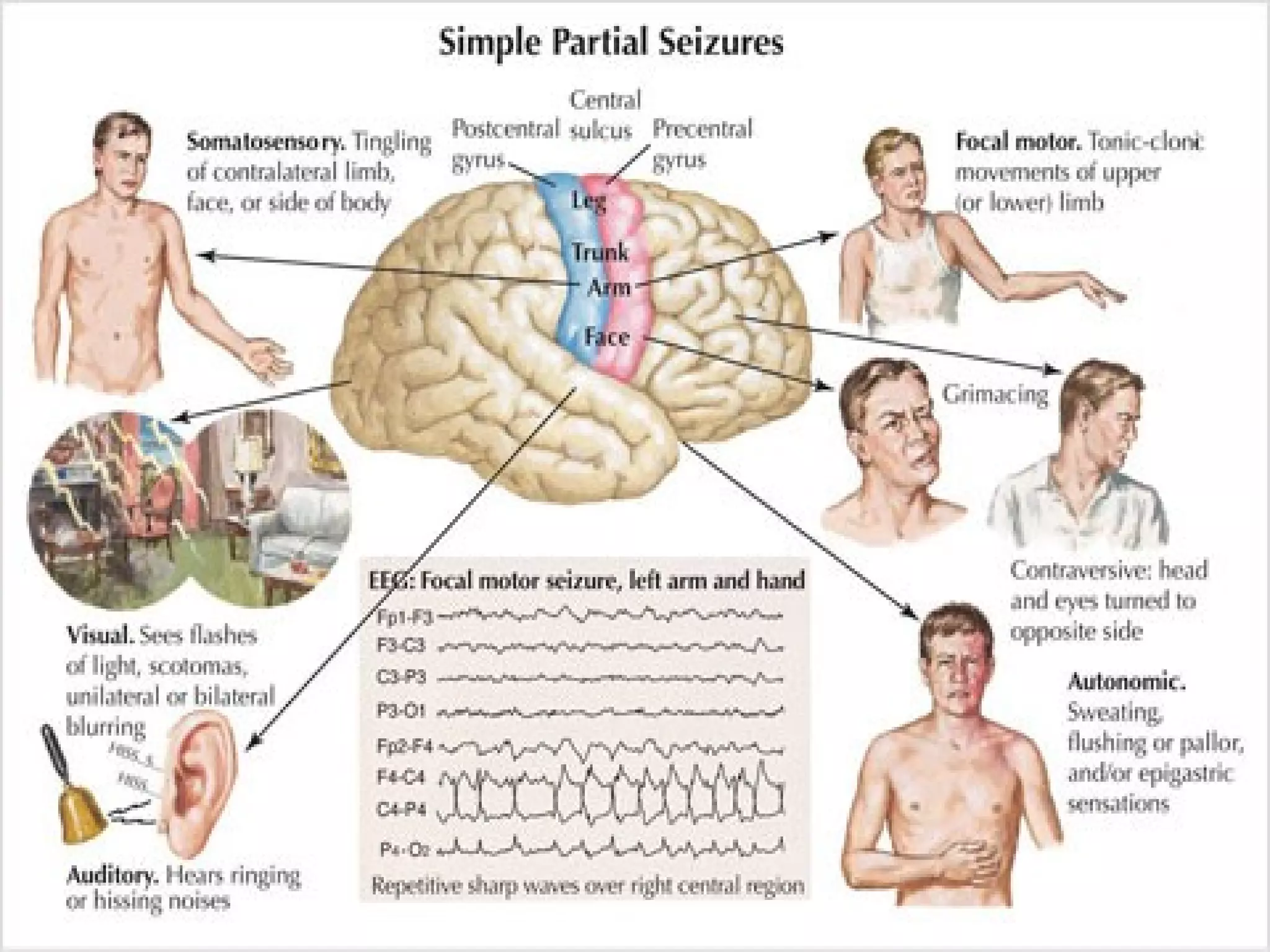
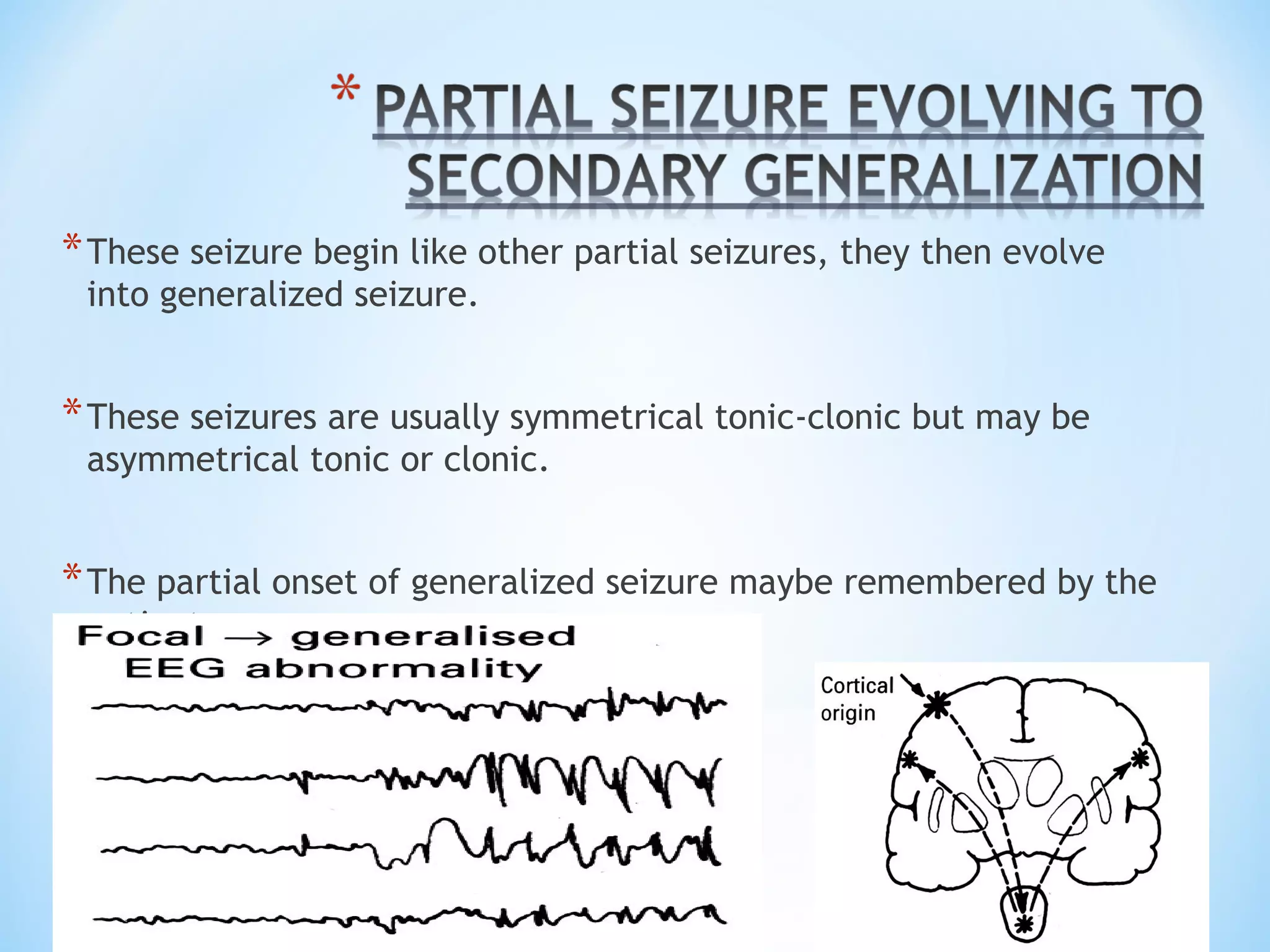
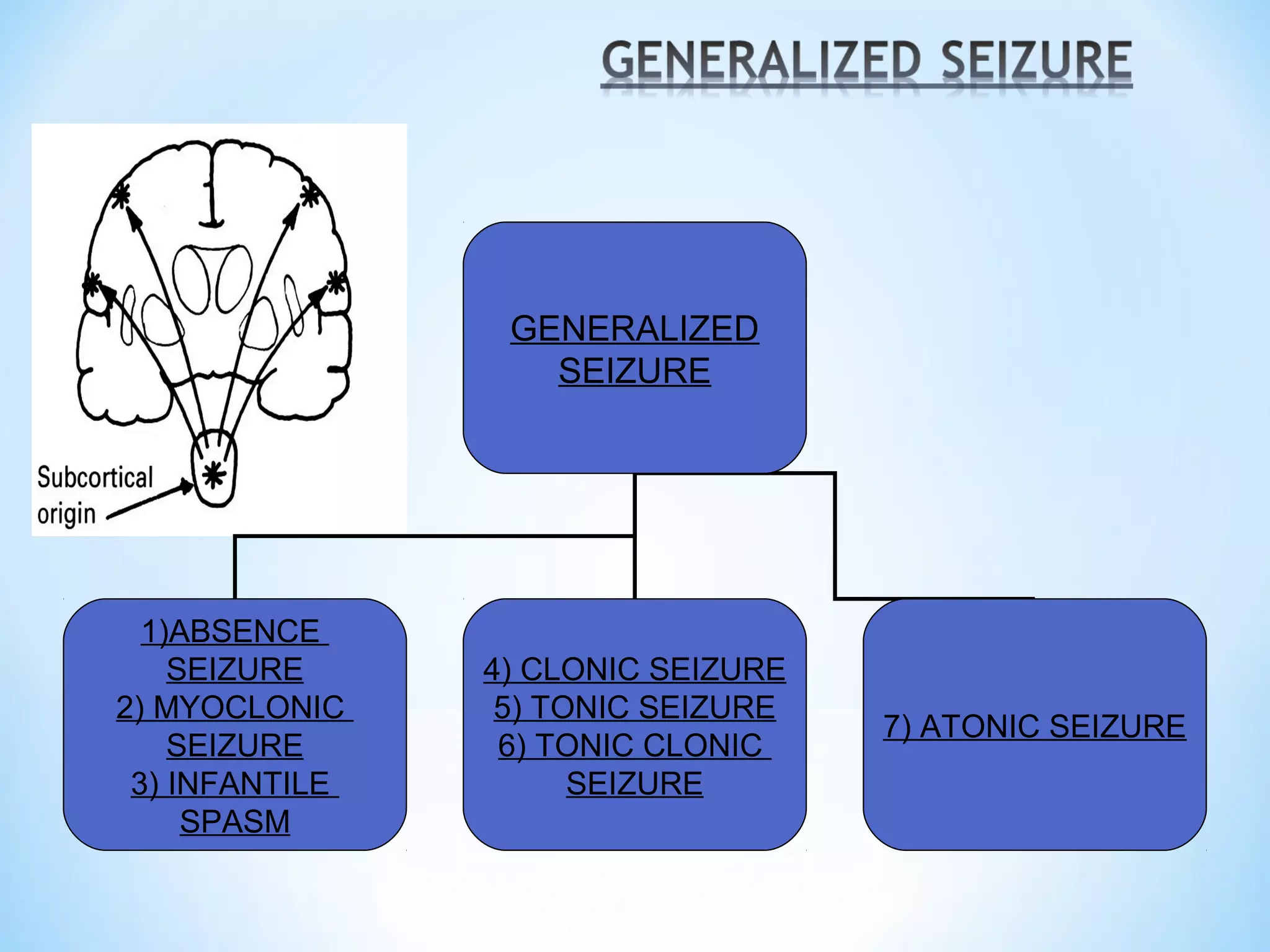
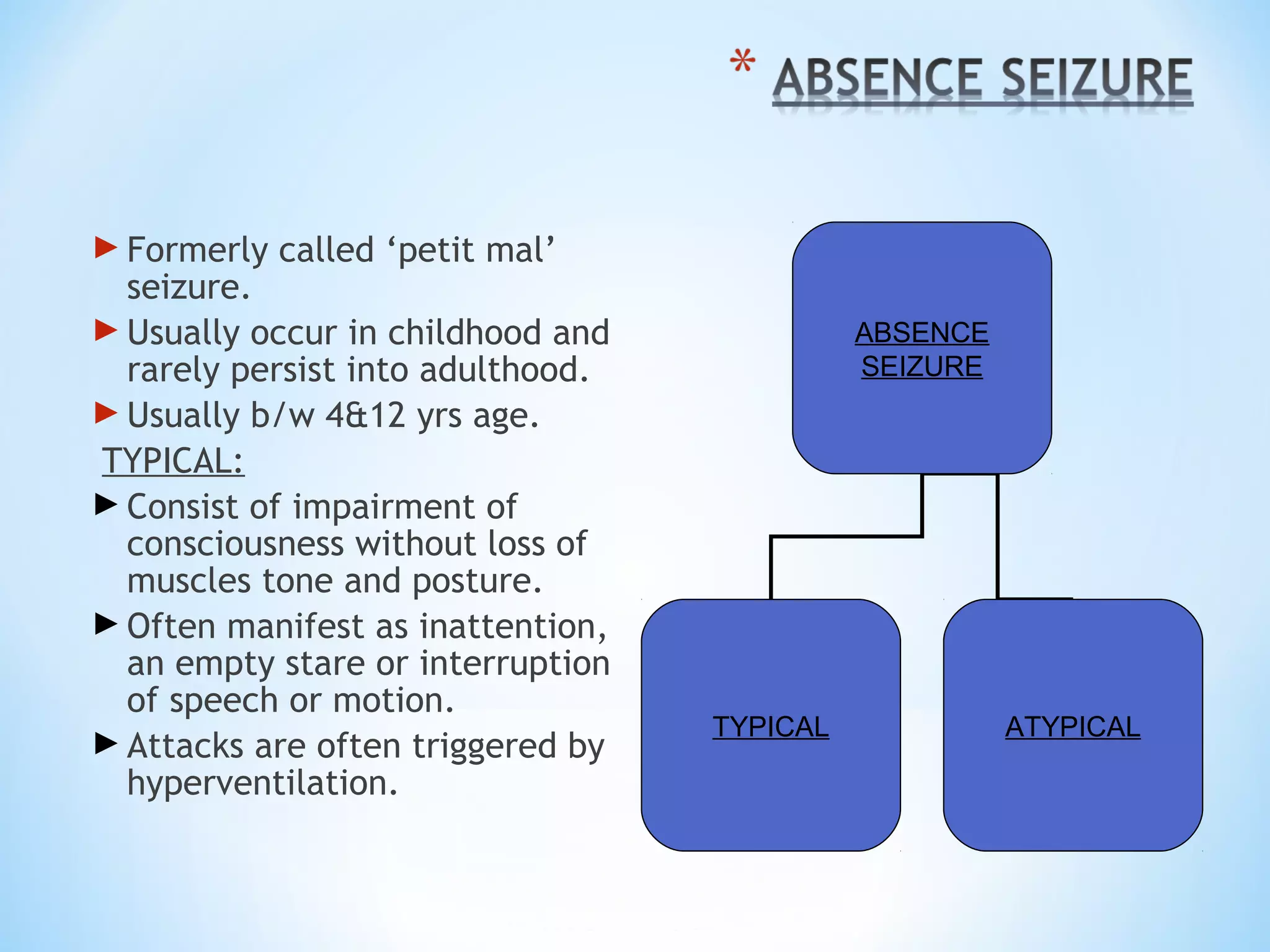
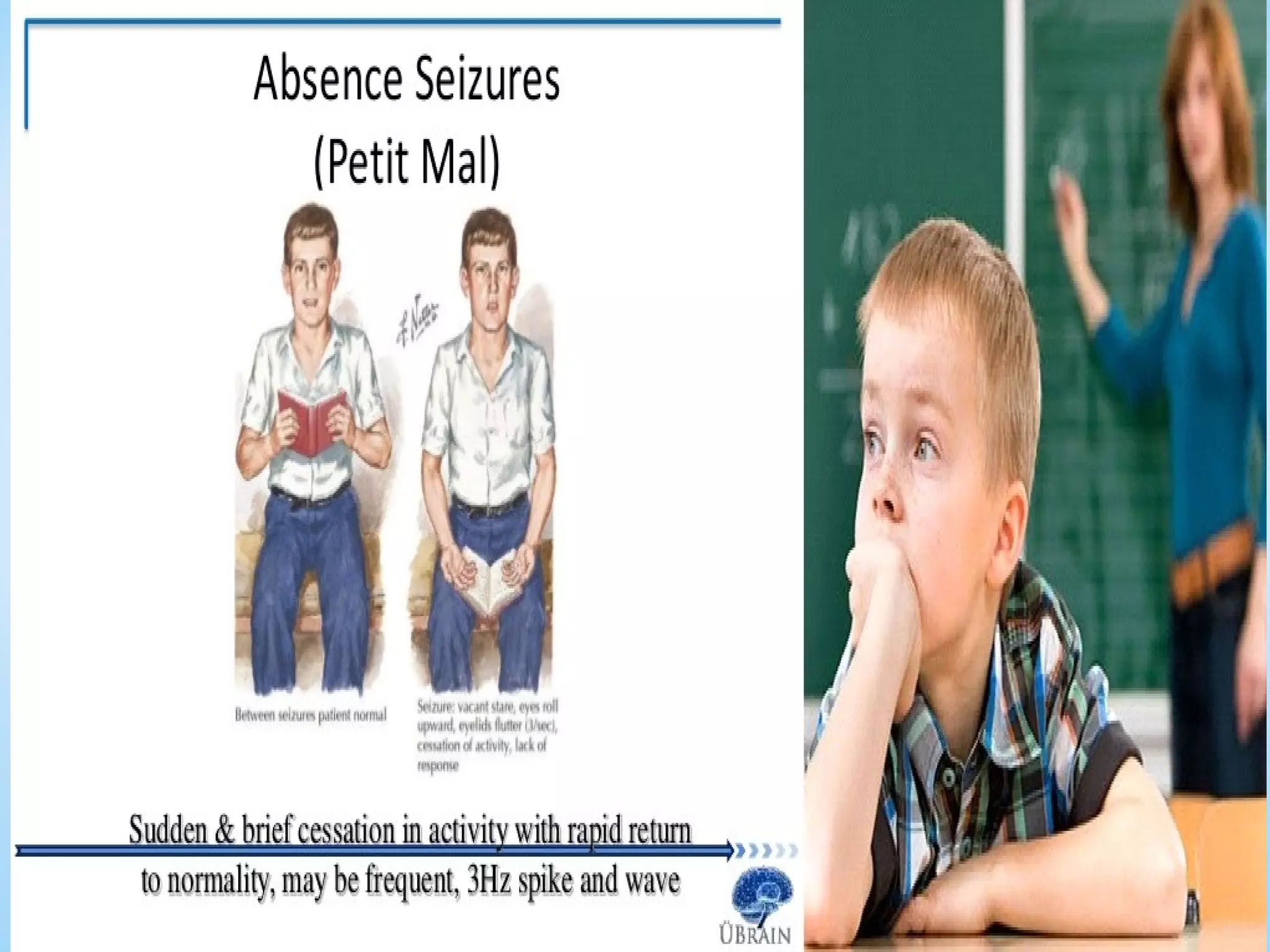
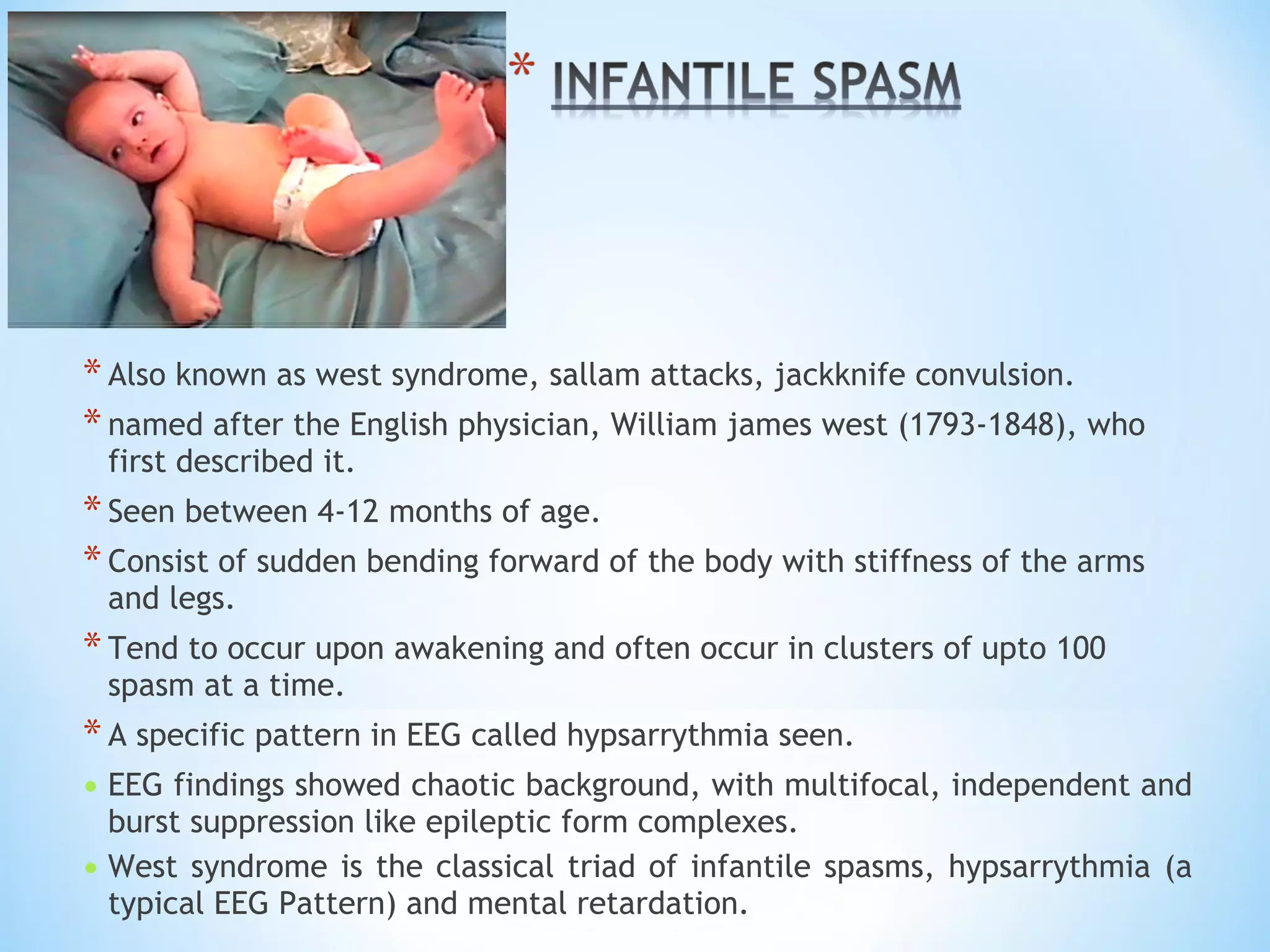
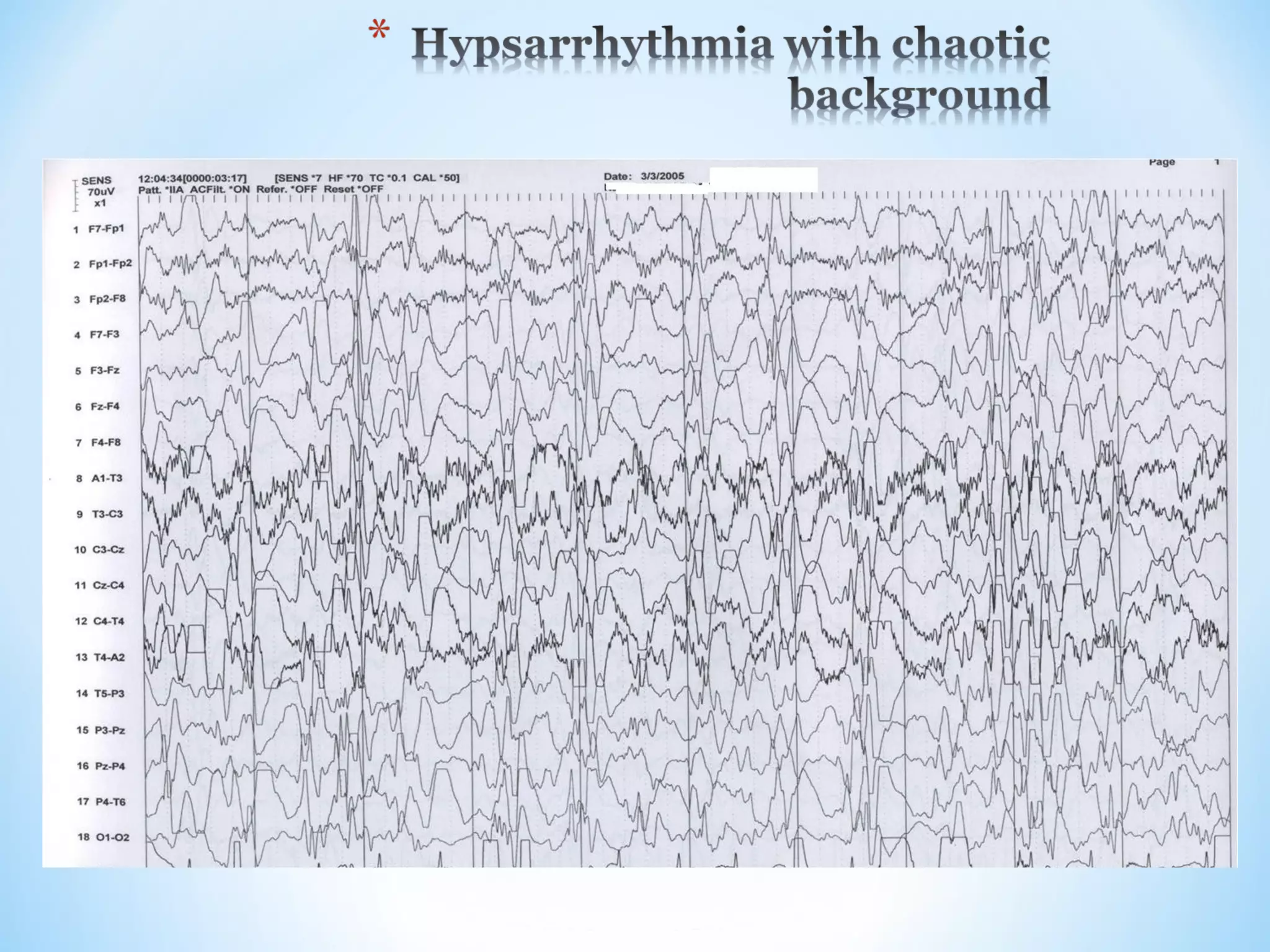
This document discusses different types of seizures, including partial seizures (simple and complex), generalized seizures (absence, myoclonic, infantile spasms, clonic, tonic, tonic-clonic, atonic), and provides details on each type. It also covers topics like epilepsy, seizure classification, recognizing seizures, and complex partial seizures transitioning to generalized seizures.