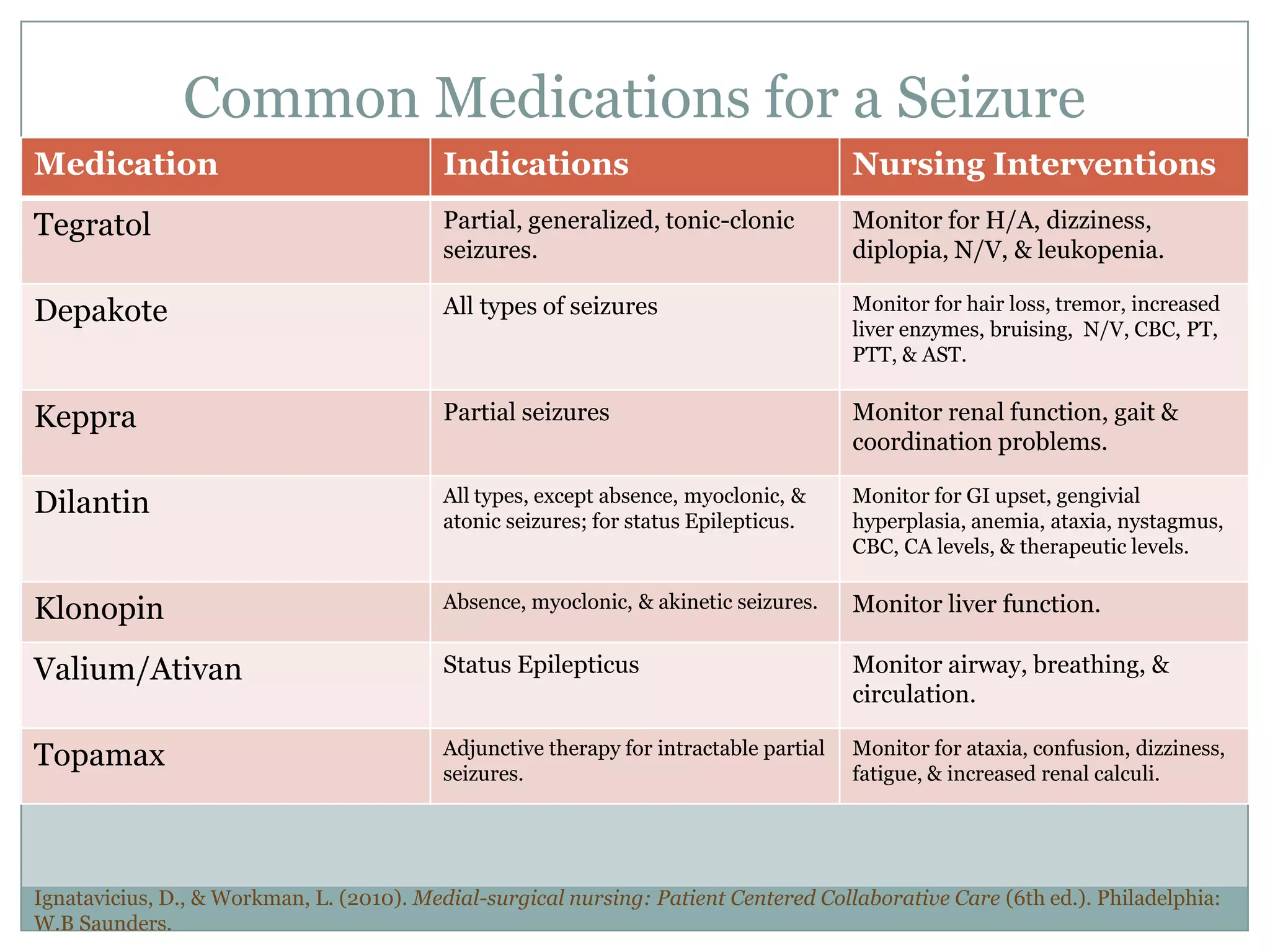
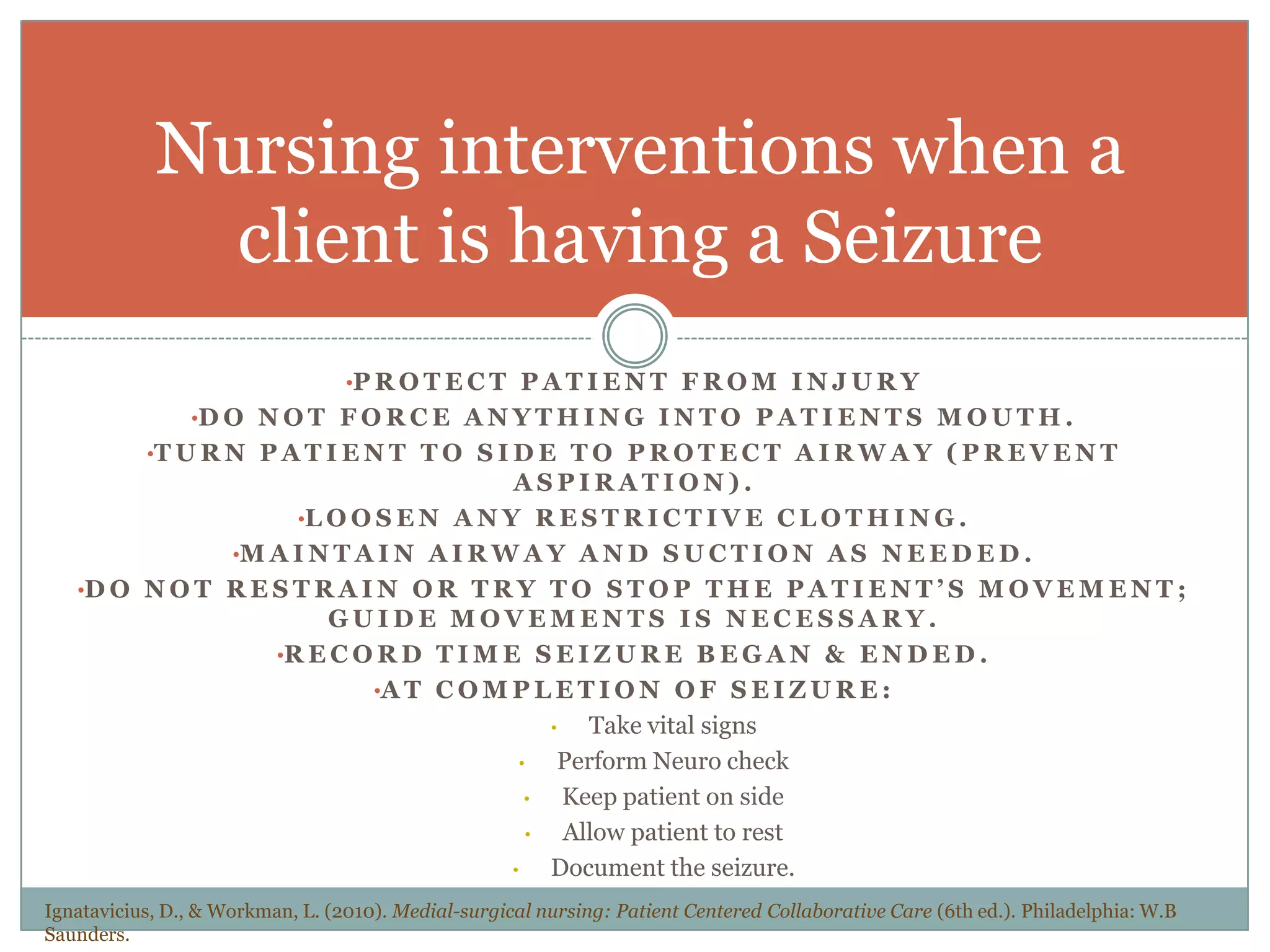
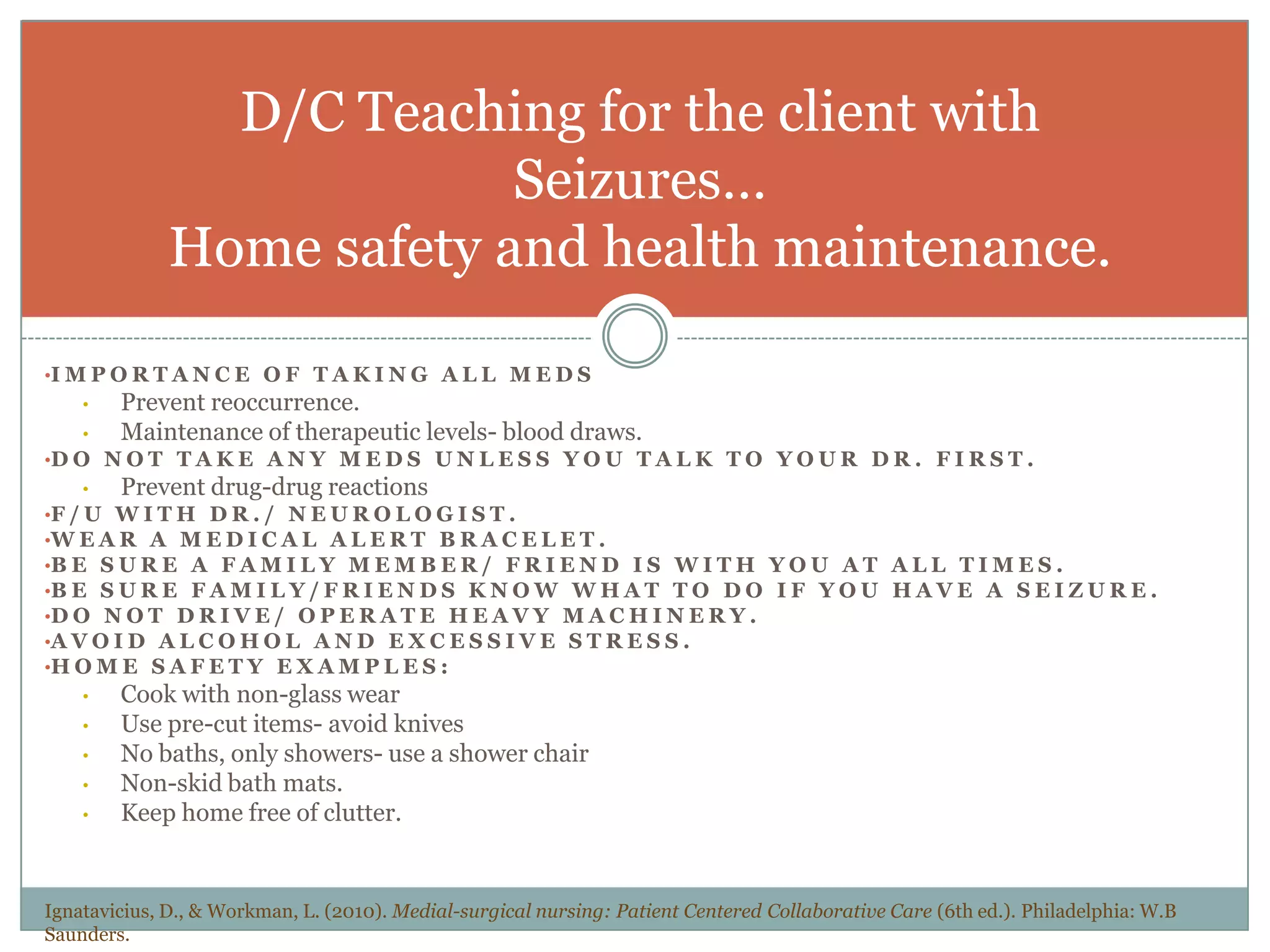
A nurse is providing report on a client admitted with seizures. The nurse discusses the pathophysiology and causes of seizures, including types like tonic-clonic and absence seizures. Common anti-seizure medications are also mentioned. Nursing interventions during a seizure include protecting the airway and preventing injury, as well as post-seizure neuro checks and rest. Discharge teaching stresses medication compliance, follow up, lifestyle modifications, and home safety precautions.