Downloaded 203 times
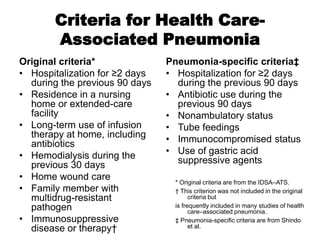
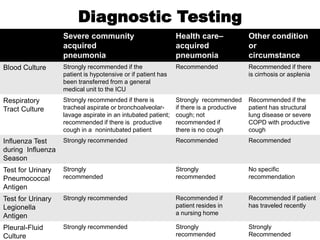
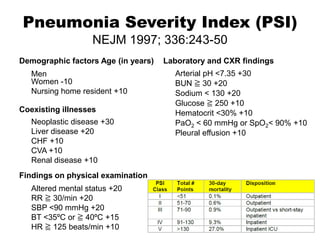
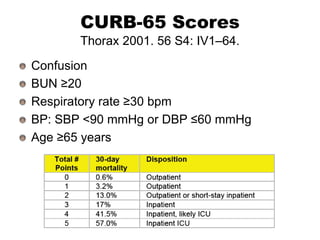
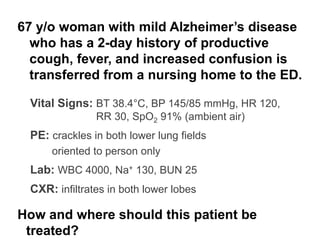
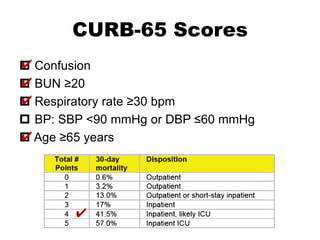
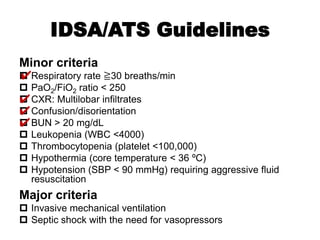
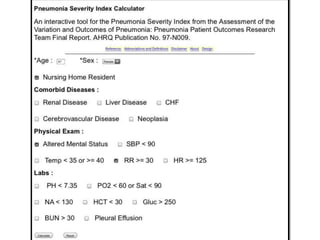
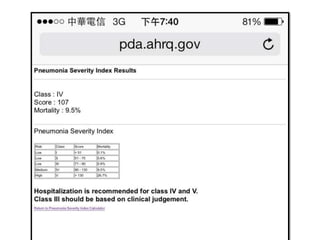
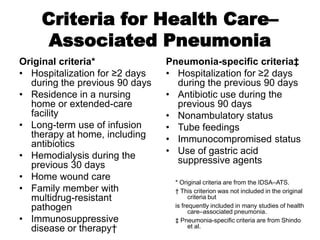


This 67-year-old woman with mild Alzheimer's disease presents with community-acquired pneumonia based on symptoms of productive cough, fever, confusion and exam findings of crackles in both lower lung fields and CXR infiltrates. She meets 3 CURB-65 criteria (confusion, RR≥30, age≥65) and 4 IDSA-ATS minor criteria (RR≥30, confusion, BUN>20, PaO2/FiO2<250) warranting consideration of ICU admission given risk of deterioration. Based on her nursing home residence and recent hospitalization, she also meets criteria for possible healthcare-associated pneumonia and should receive broad-spectrum antibiotics with MRSA and Pseudomonas coverage along with diagnostic

























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




