Downloaded 498 times

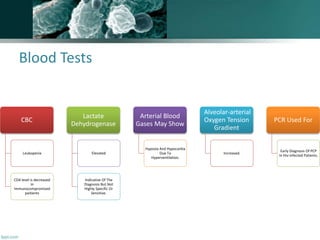
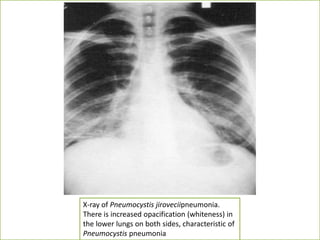

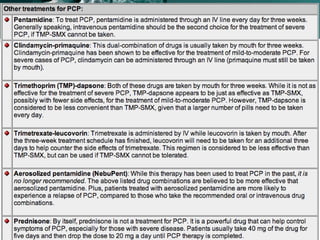


A 30-year-old man from Yemen presented with fever and dyspnea for three weeks. He had a history of occasional smoking and unclear sexual history. On examination, he had rapid breathing and oxygen saturation of 91% on room air. Initial tests showed leukopenia and elevated LDH. Chest X-ray showed diffuse bilateral infiltrates. Given his symptoms and test results, Pneumocystis pneumonia was suspected as the cause of his dyspnea. Treatment with trimethoprim-sulfamethoxazole was recommended, with alternatives available for patients with sulfamethoxazole allergy.























































































