Downloaded 25 times

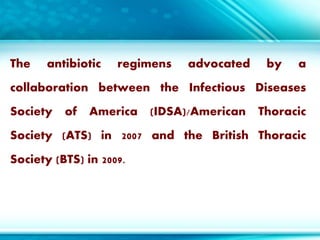

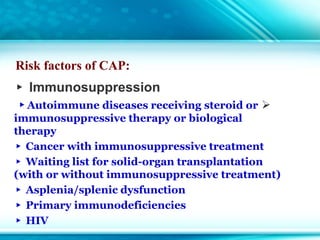
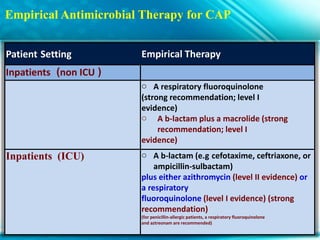
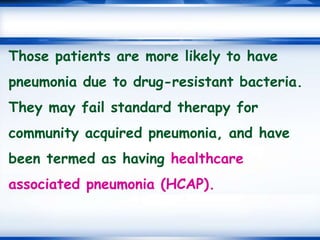
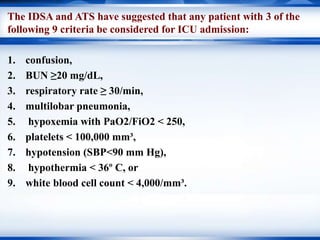
![Empirical Antimicrobial Therapy for CAP
Patient Setting Empirical Therapy
Outpatients
Previously healthy and no use of
antimicrobials within the
previous 3 months
o Macrolide (strong
recommendation; level I evidence)
o Doxycyline (weak
recommendation; level III
evidence)ycycline
Presence of comorbidities such as
chronic heart, lung, liver
or renal disease; diabetes mellitus;
alcoholism; malignancies;
asplenia; immunosuppressing
conditions.
o A respiratory fluoroquinolone
(moxifloxacin, gemifloxacin, or
levofloxacin [750 mg]) (strong
recommendation; level I
evidence)
o A b-lactam plus a macrolide
(strong recommendation; level
Ievidence)](https://image.slidesharecdn.com/cap-180312080631/85/Update-management-of-CAP-37-320.jpg)
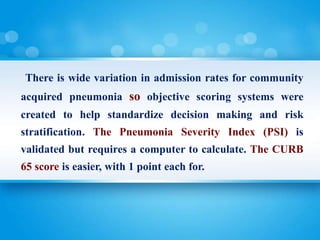
![The use of systemic corticosteroids in
patients with CAP
may reduce the length of time until
clinical stability, reduce hospital length
of stay, reduce the need for mechanical
ventilation, and reduce the incidence of
adult respiratory distress syndrome
(ARDS). [49, 50] Recent clinical trials
have also shown a possible overall
reduction in mortality, although these
later results remain in doubt. [51, 52]
Furthermore,](https://image.slidesharecdn.com/cap-180312080631/85/Update-management-of-CAP-51-320.jpg)


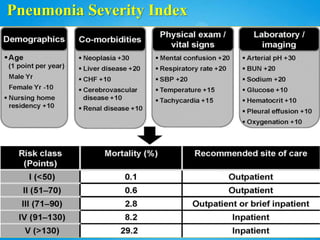
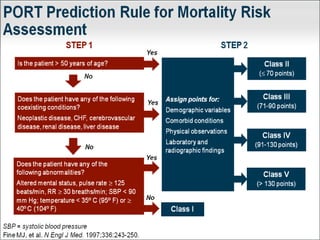
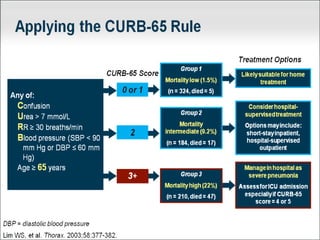
Community-acquired pneumonia (CAP) is a common infectious disease worldwide and a major cause of mortality and morbidity. The document discusses definitions, etiology, risk factors, diagnosis, and treatment recommendations for CAP according to guidelines from IDSA/ATS. Key points include common bacterial and atypical pathogens causing typical and atypical CAP; use of severity assessment scores to determine hospitalization and ICU needs; recommendations for empirical antibiotic therapy based on patient factors; and considerations for MRSA coverage and broad-spectrum therapy.





















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)