Downloaded 86 times



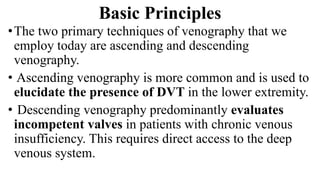

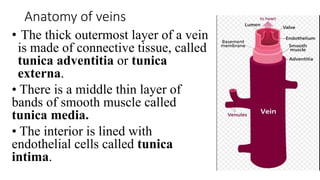
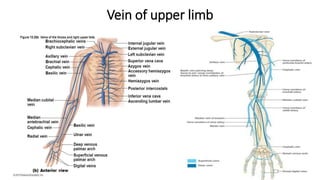



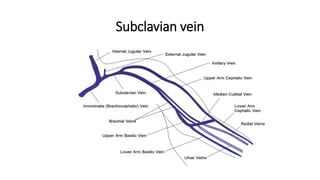
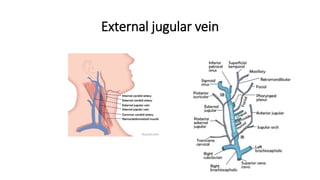
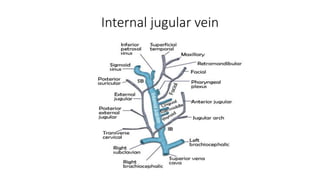
















































This document provides an overview of venography, which is an imaging technique used to examine veins. It discusses the basic principles of venography, including ascending and descending techniques. It describes the anatomy of veins and provides diagrams. It also covers indications, contraindications, techniques, and potential complications of lower limb, upper limb, and peripheral varicography venography procedures. The goal of venography is to accurately diagnose conditions like deep vein thrombosis.














































































