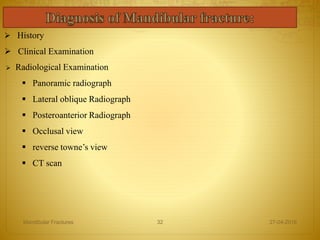
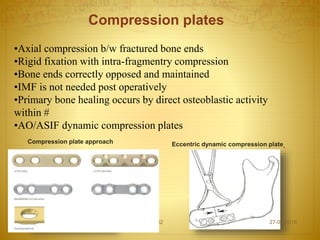
The document discusses the history, anatomy, classification, examination, diagnosis, and treatment of mandibular fractures. It traces the history from descriptions in ancient texts to modern techniques. The mandible has a unique anatomy as a bent bone that provides both compression and tension zones. Fractures are classified in various ways including by location, number of fragments, involvement of surrounding tissues, and relation to occlusion. Clinical examination involves inspection, palpation, and neurological and range of motion tests while radiographs help confirm and characterize fractures.


![ 3-D plate osteosynthesis; Dental Research Journal /Mar 2012 /Vol 9 /
Issue 2
R. Mukerji , G. Mukerji , M. McGurk Mandibular fractures: Historical
perspective British Journal of Oral and Maxillofacial Surgery 44 (2006)
222–228
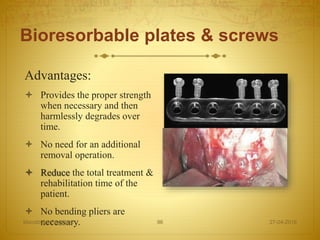
Bioresorbable plates & screws[Robert M. Laughlin JOMS
2007;65:89-96]
Killey & kay textbook of mandibular fractures.
27-04-2016Mandibular Fractures 114](https://image.slidesharecdn.com/mandibular-160427140703/85/Mandibular-fractures-114-320.jpg)